
ECR 2018 / C-1429

What you see is NOT what you get: Imaging differentials of diplopia.
Congress:
ECR 2018
Poster Number:
C-1429
Type:
Educational Exhibit
Keywords:
Education and training, Diagnostic procedure, Computer Applications-Detection, diagnosis, MR-Spectroscopy, MR-Angiography, MR, Neuroradiology brain, Eyes, CNS
Authors:
S. Neelakantan, A. Anil Kumar; Bangalore/IN
DOI:
10.1594/ecr2018/C-1429

Table 2:
Regions of interest with optimum imaging strategies for evaluation of diplopia.
. “Humming bird sign” is also noted with flattening or concave outline to superior aspect of midbrain which should be upwardly convex (white arrow) .
Diagnosis was progressive supra nuclear palsy (PSP).
References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 8:
Patient with impairment of cognition, abnormal eye movements and disturbances...
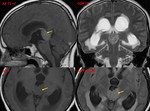
Fig. 9:
Patient presenting with parinaud syndrome.
MR images shows a well defined, T1...
 and superior cerebellar artery, draining into multiple prominent venous structures, thence to the superior sagittal sinus, right transverse sinus and peri sylvian veins and through multiple trans medullary veins into superior sagittal sinus. MR images shows dilated flow voids (yellow arrow) in the pineal region with oedema within the right mibrain/ pons. References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 10:
There is evidence of a compact high-flow AVM in the region of posterior third...

Fig. 11:
24 year old male presenting with slowly progressive motor weakness and temporal...
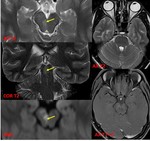
Fig. 12:
Patient with diplopia with right third nerve palsy and left sixth nerve palsy...
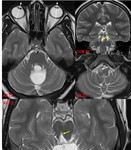
Fig. 13:
Patient with history of surgery for a posterior third ventricular arachnoid...
 in the right midbrain with significant blooming on susceptibility weighted images. Suggestive of a cavernoma. References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 14:
Patient with downgaze diplopia clinically with right trochlear nerve palsy . MR...

Fig. 15:
25 year old male with fever and headache for 20 days and left lateral rectus...
. References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 16:
Patient with left sided ophthalmoplegia. Left superior cerebellar artery...

Fig. 17:
Patient with right sided ophthalmoplegia with an extra axial right CP angle...

Fig. 18:
25 year old male with severe headache for 3 moths associated with vomiting and...

Fig. 19:
Patient with left sided facial pain, muscle wasting and diplopia.MR images...
 T1 hypo intense, T2 hyper intense, homogenously enhancing lesion (arrow) with no susceptibility artefacts on SWI imaging. Histopathology indicated that the lesion was a left cavernous sinus haemangioma. References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 20:
Patient with diplopia for 1 year. MR images shows a left para sellar (with...
. Bilateral acoustic schwannomas (orange arrow) and spinal extramedullary neurofibromas (white arrow) were also noted. HPE correlation showed a cavernous sinus meningioma. References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 21:
Known case of neurofibromatosis type 2 with right sided third nerve palsy. MR...

Fig. 22:
33 year old female with headache and diplopia with ptosis of left eye for 20...

Fig. 23:
43 year old female, diabetic with sudden pain, lateral deviation and proptosis...

Fig. 24:
17 year old male presented with history of trauma followed by pain, proptosis,...
.
Features are suggestive of an En plaque meningioma.
References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 25:
Patient with right sided ophthalmoplegia. MR images showed an ill defined...
. Suggestive of Tolosa- Hunt syndrome. References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 26:
48 year old female presenting with right abducens nerve palsy and right sided...
. The fracture line is noted extending across the sphenoid bone (white) to the contralateral anterior clinoid process. References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 27:
Patient with history of trauma CT shows a mildly displaced fracture of the roof...

Fig. 28:
Patient with right sided proptosis and diplopia. MR images showed a well...
 along the right medial orbital wall encasing the medial and inferior rectus muscles. Symptoms improved on steroids. Diagnosis was inflammatory pseudotumour. References: Department of Radiology, SSSIHMS, Bangalore")
Fig. 29:
Patient with right sided proptosis and diplopia. MR images showed an intensely...