INTRODUCTION
The CS is an uncommon imaging finding in hepatic lesions,
although is found in a variety of liver pathologies ranging from benign to malignant tumors.
It is considered to be a discriminatory feature for the positive and differential diagnosis of liver masses with a different therapeutic approach.
The most common liver masses associated with a CS are represented by:
- focal nodular hyperplasia (FNH)
- large hemangioma
- fibrolamellar carcinoma (FLHC) [1].
Rarely,
a CS has been described in other hepatic tumors such as:
- hepatocellular carcinoma (HCC)
- peripheral type cholangiocarcinoma
- some hepatic metastases [2].
CLINICAL AND LABORATORY FINDINGS guiding the diagnosis of HT with CS
The patient's clinical history,
laboratory findings and epidemiological factors can play an important role in the imaging differential diagnosis of HT with CS,
especially when different pathologies such as vascular,
metabolic,
infectious or neoplastic processes which primarily or secondarily affect the liver,
may represent risk factors in developing specific types of tumors ( Fig. 1 ).
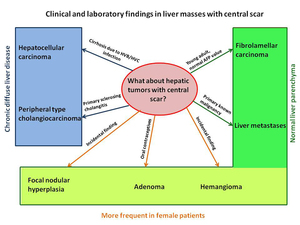
Fig. 1: Clinical and laboratory findings in hepatic tumors with central scar
References: Radiology and Imaging Department, Fundeni Clinical Institute, Bucharest, Romania
Primary hepatic malignancies with CS appear more frequently in the presence of chronic diffuse liver disease such as liver cirrhosis,
hemochromatosis and steatohepatitis,
with the exception of fibrolamellar carcinoma which affects normal hepatic parenchyma in young adults (mean age of 23 years old) [3].
In contrast,
liver metastases with a CS must be taken into account when the masses appear without a subsequent hepatic pathology,
in a patient with known primary malignancy.
The benign hepatic tumors associated with central scar such as FNH,
adenoma and giant hemangioma are more common found in female patients,
but only hepatic adenomas were related with long term use of oral contraceptives,
androgen steroid intake and glycogen storage disease [4].
THE SCAR MORPHOLOGY IN HEPATIC MASSES
Scars may be found in multiple different types of hepatic tumors and are considered to be a particular feature because of its histological nature,
which differs in each disorder (Table 1).
Table 1.
The most common hepatic scars and its particular morphology [5][6][7]
|
|
Hepatic tumors with central scar
|
Scar morphology
|
|
Most common
|
FNH
|
Fibrosis,
cholangial proliferation,
malformed vessels
|
|
Hemangioma
|
Hemorrhage,thrombosis,
hyalinization,
liquefaction,
fibrosis
|
|
FLHC
|
Fibrosis,
hemorrhage
|
|
Less common
|
HCC
|
Fibrosis,
necrosis,
fatty infiltration
|
|
Cholangiocarcinoma
|
Fibrosis,
necrosis
|
|
Metastases
|
Fibrosis,
necrosis,
hemorrhage
|
The histological nature of the central scar correlates with a particular imaging aspect including the pattern of enhancement.
Other characteristic components for scar differentiation include the size and associated findings [8].
DIAGNOSIS IMAGING
The CT and MRI exams play a defining role in the characterization of hepatic tumors with central scar,
representing a challenge for radiologists especially as most of these lesions are diagnosed based on imaging findings [7].
On CT images,
the central scar appears hypoattenuating to liver parenchyma,
with no contrast uptake or delayed enhancement.
Thus,
some specific CT criteria were found to be statistically significant in diagnosing different types of hepatic tumors with central scar,
such as:
- tumor size larger than 10cm;
- width of tumor scar;
- surface lobulation;
- calcification;
- heterogeneity;
- nodular centripetal enhancement;
- marked hyperattenuation on arterial phase images;
- isoattenuation with liver tissue on portal venous phase images;
- vascular invasion;
- extrahepatic metastases [1].
On MRI examinations,
hepatic scars appear hypo/hyperintense on T2wi,
with the same lesion enhancement patterns as on CT.
This type of investigation plays an increasingly greater role in imaging hepatic tumor,
due to the lack of using ionizing radiation and superior lesion-to-liver contrast,
improved by liver-specific contrast media administration [3].
DIFFERENTIAL DIAGNOSIS
The main differential diagnosis of CS is represented by tumor necrosis,
which is the greatest mimic (Table 2).
Table 2.
Hepatic lesions with a necrotic pseudoscar [9][10]
|
Benign hepatic lesions
|
Malignant hepatic lesions
|
|
Hepatic adenoma
FNH (very rare)
Sclerosed hemangioma
Biliary cystadenoma
Liver pyogenic infection
Post-surgical or post-radiation trauma
|
HCC/FLHC
Cholangiocarcinoma
Necrotic metastases
Biliary cystadenocarcinoma
Epitheloid hemangioendothelioma
Hepatoblastoma
Cystic sarcomas
|
On CT images,
necrosis appears as low-attenuating areas measuring between 10 and 30HU,
whereas in MRI examinations these areas appear hyperintense on T2wi and hypointense on T1wi,
both without any relevant contrast uptake [11].
TREATMENT
The accurate identification of the particular features of HT with CS,
leading to a correct imaging diagnosis,
is crucial for the subsequent therapeutic approach.
Thus,
FNH and uncomplicated liver hemangiomas and adenomas may be treated conservatively,
whereas most of the malignant tumors need an interventional or surgical approach [12].

