Skeletal manifestations in NF-1 occurs in around 25-40%. It can involve any part of the body.
These manifestations can be identified on Plain radiograph.
Spinal deformities
Spinal deformities occur in up to 50% of patients with NF-1.
One of the most common osseous complication of NF-1 is Scoliosis,
affecting 21% of patients.
Dwarfism is caused by scoliosis.
It can be dystrophic (Fig.
8) or nondystrophic (Fig.
7).
Nondystrophic scoliosis is same as idiopathic scoliosis,
but with an early onset.
It may progress to dystrophic especially when patient presents before 7 years.
Dystrophic scoliosis,
which is characteristic of NF-1,
progresses more rapidly and has a poorer prognosis.
- Sharply angled focal kyphoscoliosis (50%). (Fig.
9)
It is seen in lower thoracic and lumbar spine.
It is due to abnormal development of vertebral body.
Kyphosis often predominates over scoliosis,
incidence increases with age.
- Hypoplasia of pedicles,
transverse and spinous process.
- Scalloping of posterior vertebral margins. (Fig.
10)
It occurs due to weakened meninges allowing transmission of normal CSF pulsations which causes dural ectasia (Fig.
11) which refers to circumferential dilatation of the dural sac.
It can be associated with dystrophic skeletal changes,
potentially leading to spinal instability and angular deformity.
Posterior vertebral scalloping is common in NF-1 and is diagnosed when the depth of scalloping is greater than 3 mm in the thoracic spine or greater than 4 mm in the lumbar spine.
- Severe rotation of the Apical vertebra.
- Vertebral wedging.
- Dumbbell-shaped Enlargement of neural foramina.
- Widened interpediculated distance. (Fig.
12)
- Presence of paraspinal mass. (Fig.13)
- Spindling of the transverse process.

Fig. 7: Anterioposterior radiographs taken in 38year old NF1 patient showing nondystrophic scoliosis.
References: Department of Radiodiagnosis, Shri Sathya Sai Medical College and Research Institute, Chennai/IN

Fig. 8: Dystrophic Scoliosis
Anterioposterior radiographs Showing Increased angulation in the Thoracolumbar region and interpedicular distance is diminished in the lumbar spine
References: Yusuf AS, Pillai A, Menon SK, Panikar D. Massive spontaneous hemothorax, giant intrathoracic meningocele, and kyphoscoliosis in neurofibromatosis type 1. Journal of surgical technique and case report. 2014;6(1):33-6.

Fig. 9: Chest X-ray posterior-anterior view showing kyphoscoliosis in case of neurofibromatosis type-1
References: Sureka B, Thukral BB, Mittal MK, Mittal A, Sinha M. Imaging spectrum of neurofibromatosis. Journal of Mahatma Gandhi Institute of Medical Sciences. 2015 Jul 1;20(2):137.
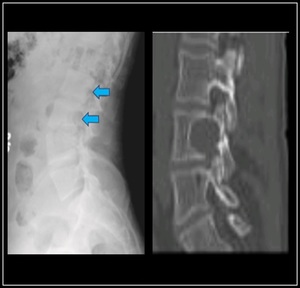
Fig. 10: Lateral radiograph of Lumbar spine showing scalloping of Posterior body wall of vertebra and CT image showing Posterior Scalloping of Vertebra
References: Sureka B, Thukral BB, Mittal MK, Mittal A, Sinha M. Imaging spectrum of neurofibromatosis. Journal of Mahatma Gandhi Institute of Medical Sciences. 2015 Jul 1;20(2):137.

Fig. 11: Sagittal T2-weighted MR image of thoracic spine taken in a case of NF1 shows posterior vertebral scalloping (arrow) along with dural ectasia.
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.
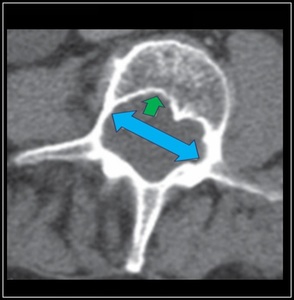
Fig. 12: Transverse CT image of lumbar spine shows thinning of pedicles, widening of interpedicular distance(blue) with posterior vertebral body scalloping(green arrow)
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.

Fig. 13: Transverse T2-weighted MR image of spine shows dumbbell neurofibroma (asterisk) expanding neural foramen and invading spinal canal.
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.
Skull
- Macrocranium and macroencephaly.
- Lleft-sided calvarial defect adjacent to lambdoid suture (Fig.14)
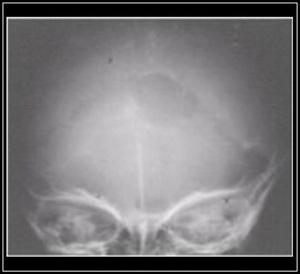
Fig. 14: Oval defect in the Labdoid suture on left.
References: Kakarla S. Skull radiographs as a guide for diagnosing systemic disorders (Pictorial Atlas). J Med Sci Res. 2016; 4(1):41-50
Orbit
- Sphenoid wing dysplasia (Fig.
15 (a) & 15 (b)) (Harlequin appearance to orbit)
It is due to failure of development of membranous bone causing partial absence of greater and lesser wing of sphenoid bone and orbital plate of frontal bone.
- Hypoplasia and elevation of lesser wing of sphenoid
- Defect in sphenoid bone with or without extension of middle cranial fossa structures into orbit.
(Fig.
16(a))
- Concentric enlargement of optic foramen.
- Enlargement of orbital margins and superior orbital fissure.
It is due to plexiform neurofibroma (Fig.16(b)) of peripheral and sympathetic nerves within orbit/optic nerve glioma.
- Sclerosis in the vicinity of optic foramen.
Caused by optic nerve sheath meningioma.
- Deformity and decreased size of ipsilateral ethmoid and maxillary sinuses.
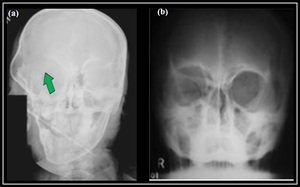
Fig. 15: (a) Skull Radiograph in NF 1 patient, Anteroposterior View Showing Right sided bare orbit with absent greater wing of sphenoid
(b) Skull Radiograph Anteroposterior view showing empty orbit sign
References: (a) Sureka B, Thukral BB, Mittal MK, Mittal A, Sinha M. Imaging spectrum of neurofibromatosis. Journal of Mahatma Gandhi Institute of Medical Sciences. 2015 Jul 1;20(2):137. (b) Kakarla S. Skull radiographs as a guide for diagnosing systemic disorders (Pictorial Atlas). J Med Sci Res. 2016; 4(1):41-50

Fig. 16: (a) NF involving left orbit and frontal bone
(b) Plexiformneurofibromatosis with sphenoid wing dysplasis
References: (a) & (b) Kakarla S. Skull radiographs as a guide for diagnosing systemic disorders (Pictorial Atlas). J Med Sci Res. 2016; 4(1):41-50
Chest Wall
- Twisted “ribbonlike” ribs in upper thoracic segments (Fig.
17)
- Inferior rib notching can occur due to multiple neurofibromas of intercostal nerves:
- Chest wall mass invading / eroding / destroying adjacent rib
- Pectus excavatum and pectus carinatum
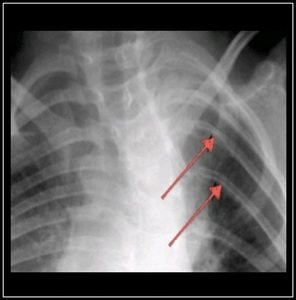
Fig. 17: 24-year-old man with neurofibromatosis type 1. Anterioposterior radiograph of ribs shows thinning of rib posteriorly, “ribbon rib” appearance (arrows).
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.
Appendicular Skeleton
- Anterolateral bowing of bone. (Fig.
18)
It can occur in variety of bone but most commonly affects lower half of tibia,
frequently fibula but very rare in upper extremity.
Tibial bowing is typically present during the first years of life before other signs of NF-1 are evident.
The bowing is characteristically anterolateral and tends to involve the distal diaphysis,
resulting in limb shortening.
Fracture typically occurs before the age of 3 years.
These are secondary to deossification causing thinning of the bone leading to pathologic fracture.
It is false joint with abnormal movement at the site of fracture and is caused by abnormal osseous remodeling.
- Nonunion after bowing fracture in 1st year of life.
It is usually seen in tibia and fibula.
- Atrophic thinned or absent fibula.
Traumatic subperiosteal hemorrhage with abnormally easy stripping of periosteum from bone.
From periosteal or soft-tissue neurofibroma (Fig.
20)
- Intramedullary longitudinal streaks of increased density
- Multiple nonossifying fibromas or fibroxanthomas
Well-defined,
expansile lucent lesions with sclerotic margins may be seen in patients with NF-1.
They are classically asymptomatic,
slightly expansile lesions occurring in the metaphysis of long bones that have a thin,
sclerotic border with a narrow zone of transition.
The presence of multiple bilaterally symmetric lower extremity nonossifying fibromas raises Fig.
26 the possibility of underlying NF-1.
It is because of deossification or nonossifying fibroma (Fig.
22)
Unilateral overgrowth of a limb bone due to overgrowth of ossification center.

Fig. 18: Child with neurofibromatosis type 1 an pseudarthrosis of tibia Anteroposterior radiograph of right leg shows Bowing of the tibia
References: Pannier S. Congenital pseudarthrosis of the tibia. Orthopaedics & Traumatology: Surgery & Research. 2011 Nov 30;97(7):750-61.

Fig. 19: Anteroposterior radiograph of left leg shows pseudarthrosis of tibia with anterior displacement of distal tibial fragment and lateral radiograph shows bowing of distal diaphysis of tibia and fibula.
References: http://www.ilizarov.org/case.asp#

Fig. 20: Anteroposterior radiograph of knee in 30-year-old, shows cortical thinning and multiple lucencies in proximal fibula and mild scallpoing of tibial cortex
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.

Fig. 21: Anteroposterior radiograph of right hip shows dysplastic acetabulum with deformity of femoral head and thinning of proximal femur in a case of neurofibromatosis 1.
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.

Fig. 22: Anteroposterior radiograph of knees shows bilateral sharply marginated lucent lesions with sclerotic margins in both distal femurs; these findings are suggestive of fibroxanthomas. Sclerosis and mild deformity of left proximal tibia were caused by prior curettage of lesion with healed pathologic fracture
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.

Fig. 23: Anteroposterior radiograph of left shoulder in a 20year old shows dysmorphic glenoid, thinning and deformity of clavicle and scapula and dislocated proximal humerus
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.

Fig. 24: Plain radiograph of forearm in 16year old boy shows hypoplasia and deformity of left radius and ulna. Intramedullary sclerotic streaks in radius and periosteal deformity seen
References: Khan AN. Neurofibromatosis Type 1 Imaging.

Fig. 25: 54-year-old woman with neurofibromatosis type 1 and cutaneous neurofibromas. Posteroanterior radiograph of left hand shows multiple cutaneous soft-tissue masses (arrows) representing neurofibromas
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.

Fig. 26: 47-year-old man with neurofibromatosis type 1 and elephantiasis neuromatosa. Posteroanterior radiograph of left hand shows diffuse soft-tissue hypertrophy; note also enlargement and mild cortical irregularity of thumb phalanges.
References: Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. American Journal of Roentgenology. 2012 Jul;199(1):W99-106.
