We have selected cases that enlighten the most important aspects of PET-CT thymus imaging and how it can contribute to an accurate diagnosis or for treatment planning.
Specifically,
we present an overview of common thymic lesions and mimics of disease,
with an emphasis on PET-CT imaging findings,
while also briefly commenting CT and MRI findings.
Cases presented include normal thymus,
thymic hyperplasia, thymic cyst,
invasive thymoma,
thymic carcinoma,
and lymphoma.
Normal appearance of thymus and variation with age
- The normal thymus is a triangular,
bilobed organ residing in the anterior mediastinum.
- Can appear quadrilateral with convex borders on young patients.
- Mild to moderate 18F-FDG uptake on young patients.
Undergoes fatty infiltration with age and progressively reduces 18-FDG uptake.
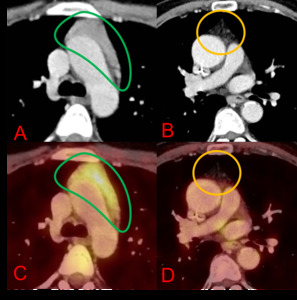
Fig. 1: Axial (A & B) CT chest and axial (C & D) PET-CT chest. 20-year-old (on the left) and 65-year-old (on the right) patients with no previous history of chemotherapy. The 20-year-old woman shows a quadrilateral thymus (green outline) with mild 18-FDG uptake (A & C), while the 65-year-old man shows a triangular thymus (orange outline) and no significant 18-FDG uptake (B & D).
Thymic hyperplasia
- Can be divided into true thymic hyperplasia and lymphoid hyperplasia (autoinmmune thymitis).
- Both entities present as diffuse symmetric thymus enlargement,
so imaging cannot reliably distinguish them.
- True thymic hyperplasia appears posterior to stressful processes,
such as chemotherapy,
corticosteroid therapy,
radiation therapy,
burns or systemic infections.
- Lymphoid hyperplasia is associated to myasthenia gravis,
systemic lupus erythematosus and Graves disease,
among other autoimmune entities.
- Thymus usually losses its bilobed appearance and appears oval in CT and shows mild increase in 18F-FDG uptake.
- A triangle shape of 18F-FDG uptake is most frequent,
but unilateral or midline patterns are possible as well.
- A SUVmax of less than 3.4 is suggestive of thymic hyperplasia,
while over 3.4 is predictive of lymphoma .
- Chemical shift MRI can be useful for differentiating thymic hyperplasia from thymic tumors.
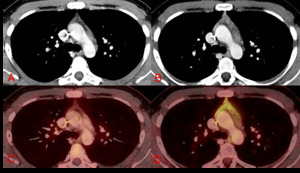
Fig. 2: Axial (A & B) CT chest and axial (C & D) PET-CT chest. A 21-year-old male underwent chemotherapy for testicular neoplasm. Pre– (A & C) and post– (B & D) chemotherapy 4 months apart images show a slight increase in thymus size and a midline-and-right-lobe pattern of 18-FDG uptake (SUV max: 3,8). A diagnosis of rebound thymic hyperplasia was made. The patient is doing fine after 2 years of follow-up.
Thymic cysts
- Can be divided into congenital cysts and adquired lesions.
Secondary lesions can appear in relation to irradiated Hodgkin’s lymphoma or in non-radiated thymic neoplasms such as thymoma or seminoma.
- Congenital cysts are unilocular lesions.
Acquired thymic cysts are usually multilocular.
- Thymic cysts usually show fluid attenuation at CT but calcifications or hemorrhage are not uncommon findings.
- Thymic cysts do not normally exhibit significant 18F-FDG uptake.
- MR imaging can be used to differentiate hemorrhagic fluid from soft tissue.
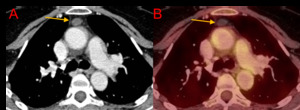
Fig. 3: Axial CT chest (A) and PET-CT chest (B). A 58-year-old female with an incidental finding of a simple appearing cyst in the region of the thymus (orange arrows); the lesion shows no significant contrast enhancement (CT density: 12 HU) nor 18F-FDG uptake. It has remained stable for 5 years and a diagnosis of thymic cyst was made.
Thymoma
- Thymomas are benign or low grade malignant tumors.
- Important association with myasthenia gravis.
- Calcifications are frequently seen in these lesions.
- Invasion of mediastinal structures,
pleural thickening,
or effusion are indicators of invasive tumor.
- Low-risk thymoma have a more heterogeneous uptake than high-risk thymoma.
- High-risk thymoma usually have a higher 18F-FDG uptake (SUVmax) than non-invasive thymomas,
however,
there is no definite SUV cut-off.
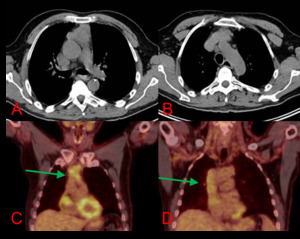
Fig. 4: Axial CT chest (A & B) and coronal (C & D) PET-CT chest. 52 year-old-male. Prevascular mass with loss of a cleavage plane concerning for vascular invasion. PET-CT shows a hypermetabolic mass (SUV max 4.5) extending through the IVC into the right atria (green arrows). Surgery confirmed findings for an invasive thymoma.
Thymic carcinoma
- Thymic carcinomas are aggressive tumors with a high tendency for distant metastasis
- Usually present on CT as multilobulated heterogenous masses with areas of necrosis and calcification
- On 18F-FDG show high uptake.
SUVmax is tipically over 7,
which can help differentiate thymic carcinoma from thymoma.
- In addition,
presence of mediastinal lymphadenopathy and distant metastasis on 18F-FDG PET-CT suggest thymic carcinoma
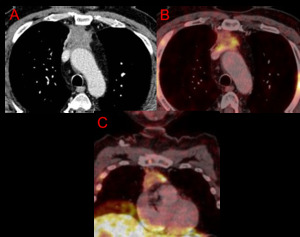
Fig. 5: Axial CT (A) and PET-CT (B) chest. Coronal PET-CT (C). Ill-defined prevascular (anterior) mass with heterogenous enhancement. PET-CT shows discrete areas of FDG uptake, yet highly metabolic at those points (SUV max 8.2). Pathology obtained at surgery revealed a thymic carcinoma.
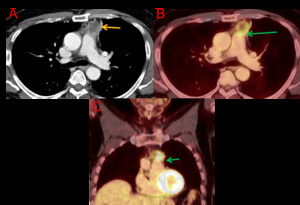
Fig. 6: Axial CT (A) and PET-CT (B) chest. Coronal PET-CT (C). 66-year-old male. Polilobulated prevascular mass with a solid peripheral contrast-enhancing component and a non-enhancing center compatible with necrotic center (orange arrow). High 18F-FDG uptake In the solid portion of the lesion (SUV max: 17.5). There is a loss of cleavage plane with the pulmonary artery on CT and PET-CT images (green arrows), as well as a subtle density of adipose tissue relative to the aortic arch, with no uptake increase. Pathology obtained at surgery revealed a thymic carcinoma.
Lymphoma
- Thymic involvement in lymphoma can occur in the setting of widespread disease or as isolated involvement.
- Hodgkin lymphoma is more frequent in this setting than non-Hodgkin’s lymphoma
- PET-CT shows a nodular,
usually asymmetrical thymus enlargement,
with SUVmax usually over 3.4
- Higher 18F-FDG uptake is suggestive of more aggressive varieties: SUVmax values over 13 are highly suggestive of aggressive lymphoma,
and less than 6 are associated with a high probability of indolent lymphoma.
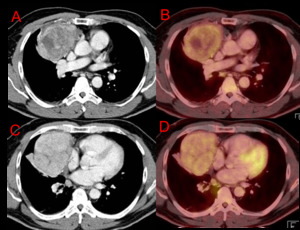
Fig. 7: Axial CT (A & C) and PET-CT (B & D) chest. Prevascular (anterior) mass with heterogenous enhancement and cystic areas within the mass. Slight uptake of FDG, with a SUV max of 4.2. Biopsy through mediastinoscopy revealed a Non-Hodgkin Lymphoma.

 CT chest and axial (C & D) PET-CT chest. 20-year-old (on the left) and 65-year-old (on the right) patients with no previous history of chemotherapy. The 20-year-old woman shows a quadrilateral thymus (green outline) with mild 18-FDG uptake (A & C), while the 65-year-old man shows a triangular thymus (orange outline) and no significant 18-FDG uptake (B & D).")
 CT chest and axial (C & D) PET-CT chest. A 21-year-old male underwent chemotherapy for testicular neoplasm. Pre– (A & C) and post– (B & D) chemotherapy 4 months apart images show a slight increase in thymus size and a midline-and-right-lobe pattern of 18-FDG uptake (SUV max: 3,8). A diagnosis of rebound thymic hyperplasia was made. The patient is doing fine after 2 years of follow-up.")
 and PET-CT chest (B). A 58-year-old female with an incidental finding of a simple appearing cyst in the region of the thymus (orange arrows); the lesion shows no significant contrast enhancement (CT density: 12 HU) nor 18F-FDG uptake. It has remained stable for 5 years and a diagnosis of thymic cyst was made.")
 and coronal (C & D) PET-CT chest. 52 year-old-male. Prevascular mass with loss of a cleavage plane concerning for vascular invasion. PET-CT shows a hypermetabolic mass (SUV max 4.5) extending through the IVC into the right atria (green arrows). Surgery confirmed findings for an invasive thymoma.")
 and PET-CT (B) chest. Coronal PET-CT (C). Ill-defined prevascular (anterior) mass with heterogenous enhancement. PET-CT shows discrete areas of FDG uptake, yet highly metabolic at those points (SUV max 8.2). Pathology obtained at surgery revealed a thymic carcinoma.")
 and PET-CT (B) chest. Coronal PET-CT (C). 66-year-old male. Polilobulated prevascular mass with a solid peripheral contrast-enhancing component and a non-enhancing center compatible with necrotic center (orange arrow). High 18F-FDG uptake In the solid portion of the lesion (SUV max: 17.5). There is a loss of cleavage plane with the pulmonary artery on CT and PET-CT images (green arrows), as well as a subtle density of adipose tissue relative to the aortic arch, with no uptake increase. Pathology obtained at surgery revealed a thymic carcinoma.")
 and PET-CT (B & D) chest. Prevascular (anterior) mass with heterogenous enhancement and cystic areas within the mass. Slight uptake of FDG, with a SUV max of 4.2. Biopsy through mediastinoscopy revealed a Non-Hodgkin Lymphoma.")