- Salient updates in the 5th edition of BI-RADS pertaining to mammography,
ultrasonography (US),
and magnetic resonance (MR) imaging will be outlined.
- Relevant features that require consideration during image interpretation and reporting as per the 5th edition of BI-RADS,
will be highlighted.
- The implications of these modifications on patient management will be emphasized.
Updates pertaining to Mammography
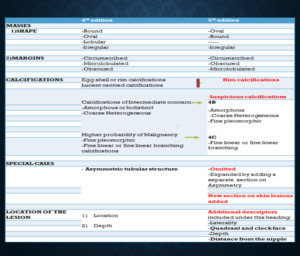
Fig. 1: The table provides an overview of the salient updates in the 5th edition BI-RADS mammography lexicon.
MASSES
- 'The term ‘lobular’ in the 4th edition of BIRADS was intended to be applied to masses with an ‘undulating’ contour.
In clinical practice,
confusion arises as the term ‘‘lobular’’ is usually applied to convey a benign etiology. Lobular has been removed from the descriptors while retaining the margin descriptor ‘‘micro lobulated’’ which implies a suspicious finding.
[1]
- The descriptors have been rearranged in order of the least suspicious morphology to the one that is most suggestive of malignancy.
Thus a circumscribed lesion is associated with the least risk of malignancy while the presence of micro-lobulations can be viewed with suspicion.
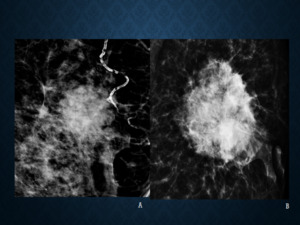
Fig. 2: Figures A and B reveal two lesions with microlobulated margins. The term ’lobular’ – previously used as a descriptor for shape has been omitted from the lexicon as it denotes a ‘benign’ lesion and is not to be confused with the term ‘micro-lobulated’ –a descriptor for margins, which denotes a suspicious lesion.
CALCIFICATIONS
- The term ‘‘rim’’ calcification typically denotes the presence of calcium surrounding a lucent center,
a finding common to the previously used terminologies of ‘egg-shell’ and ‘lucent-centred’ calcifications.
The updated lexicon eliminated these terms,
keeping a single common terminology of ‘rim’ calcifications.
The aim of this change was to simplify reporting,
as all three appearances are typically benign,
indicating fat necrosis or calcified cysts.
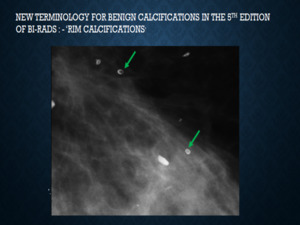
Fig. 3: The green arrows indicate ‘rim calcifications’, the new terminology for benign calcifications in the updated BIRADS lexicon, which includes ‘egg shell’ and ‘lucent centred’ calcifications indicating benign pathologies such as ‘fat necrosis’ or ‘calcified cysts
- Further simplification of the lexicon was possible,
after multiple studies deciphered the risk of malignancy for various patterns of calcification.
In accordance with these findings,
currently ‘‘amorphous’’,
‘‘coarse heterogeneous’’,
and ‘‘fine pleo-morphic’’ calcifications are considered to represent a lower risk of malignancy and are to be assigned to category 4B since the probability of malignancy is relatively low (27% for ‘amorphous calcifications,
13% for ‘‘coarse heterogeneous’’ and 50% for fine pleo-morphic’’ calcifications.) as opposed to ‘‘fine linear or fine-linear branching’’ calcifications,
with a high probability of 78% which should be assigned to category 4C. [2]
- These modifications permit appropriate malignancy risk stratification in practice,
which ultimately leads to appropriate patient management,
including planning follow-up strategies after biopsy or surgery.
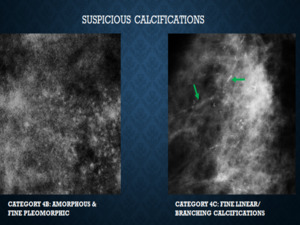
Fig. 4: Figure 4 demonstrates ‘suspicious ‘calcifications which includes categories 4B and categories 4C as per the 5th edition of BI-RADS. Improved risk stratification is now possible based on the morphology of calcifications. Secondly all of these require a tissue diagnosis, thus classifying them under one main heading simplifies management.
EXPANSION OF SECTION ON ‘ASYMMETRY’
- ‘Asymmetry’,
a term unique to the mammography lexicon,
denotes a finding seen originally on only one standard screening view,
which might later be described as a focal asymmetry if further work-up depicts the abnormality on an additional projection.
- Of greater significance is the concept of “developing asymmetry” a term proposed by Leung and Sickles in 2007,
and now included in the fifth edition of the Breast Imaging Reporting and Data System ( BI-RADS) atlas.
BI-RADS) atlas.
- Definition: A focal asymmetry that either is new or has increased in size or conspicuity compared with images from previous examinations.
- The risk of malignancy associated with a developing asymmetry is 12.8% when seen at screening mammography and a 26.7% when it persists at diagnostic mammography thus entitling the entity for a category 4 classification.
Therefore,
biopsy should be recommended for all cases of developing asymmetry.
[3]
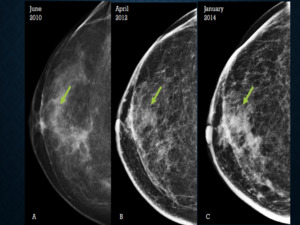
Fig. 5: Figure 5 illustrates ‘developing asymmetry’now included in the 5th edition of BIRADS. Figures A, B, and C reveal a focal asymmetry in the retro-areolar region of the right breast (arrows), on the CC view that has increased in size and conspicuity on subsequent examinations. Final diagnosis on histopathology was invasive ductal carcinoma.
OTHERS
- Additional descriptors have been included under the heading ‘location of the lesion’ such as the quadrant,
clock position and distance from the nipple,
so as to provide more clarity to the clinician,
facilitate correlation of findings seen on various imaging modalities and reduce ambiguity in radiology reports.
UPDATES PERTAINING TO ULTRASONOGAPHY
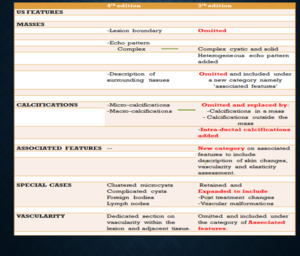
Fig. 6: The table provides an overview of the salient updates in the ultrasonography lexicon.
MASSES
- To this end,
the historic descriptor of ‘‘lesion boundary’’ has been removed from the new version of the lexicon.
This is based on the observation that the presence of echogenic rim versus an abrupt margin,
is insensitive to distinguish benign from malignant masses.
‘Lesion boundary’ has been deemed irrelevant in lesion characterization.
- The echo pattern of the mass,
was expanded to include the term ‘heterogeneous’ echo pattern’ and the term ‘complex’ echotexture was clarified and a new description was created namely ‘complex solid and cystic’.
The aim of this modification was to distinguish benign pathologies such as an abscess,
which would be classified under ‘complex solid and cystic’ while a lesion suspicious for malignancy would then be described to have a ‘heterogeneous’ echo pattern.
This provides greater clarity with regard to the index of suspicion of the lesion.
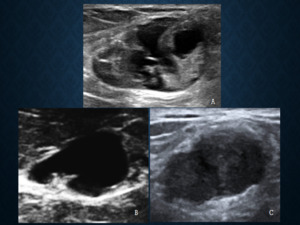
Fig. 7: The terminology ‘complex’ echo pattern (figure A) is replaced by the terms ‘complex cystic and solid’ (figure B)denoting inflammatory lesions and the term ‘heterogeneous’ echo pattern (figure C) has been added to denote lesions with a high index of suspicion.
- The change from ‘surrounding tissues’ to ‘associated features’ aligns the lexicon in a similar manner to the descriptors available within mammography and includes skin changes,
vascularity,
assessment on elastography.
[4]
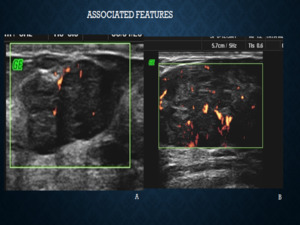
Fig. 8: A separate section on ‘associated features’ has been added which includes descriptions of ‘vascularity’ and ‘elasticity’. These supplementary features play an important role for upgrading or downgrading the BIRADS category, particularly in BIRADS 3 and 4a lesions. Figure A shows a darkly hypoechoic lesion showing mild internal vascularity, favouring benign etiology thus categorised as a BIRADS 3 lesion. While the lesion shown in figure B appears similar in morphology however shows marked internal vascularity and was categorised as BIRADS 4a. The lesion in figure A was a histopathologicaly proven fibroadenoma and the lesion in figure B turned out to be a Phyllodes tumour.
ELASTOGRAPHY
- In addition to the describing the morphology of the lesion in terms of its shape,
orientation,
margin,
echo pattern,
posterior acoustic features and additional evaluation of its elasticity is recommended.
Using the elastographic criteria,
the lesions are to be classified as soft,
intermediate,
or hard as per the new lexicon. The inclusion of elastography serves a valuable tool to re-classify indeterminate lesions,
for instance lesions that are classified as BI-RADS category 4a.
The lesions which meet most of the criteria for benign lesions,
but would benefit from further investigation with diagnostic methods or short-term follow-up may be re-classified as category 3 if determined to be ‘soft’ with the assessment of elasticity thus avoiding biopsies.
[5]
- For higher category lesions i.e.
categories 4b,
4c,
and 5,
elastography would not significantly impact management since the morphology of these lesions remains the most relevant criterion in practice when malignancy is suspected.
However elastography may provide some clues to the histology of the lesion e.g.
mucinous carcinoma,
and papilliferous carcinoma appear soft in elastography.
- Addition of elastography is aimed to improve the specificity and diagnostic accuracy of ultrasound.
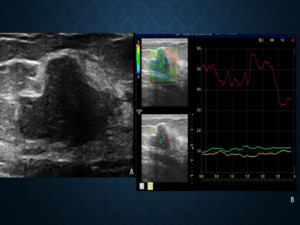
Fig. 9: Findings on elastography are now included in the lexicon to aid better risk stratification of lesions on ultrasound. Figure A reveals a darkly hypoechoic lesion seen in the right breast of a 56 year old lady. No prior ultrasound examination had been performed. On elastography, the lesion appeared predominantly soft , favouring a benign etiology. The lesion was then categorised as a BIRADS 3 lesion, which remained stable on follow up.
OTHERS
- The updated lexicon on ultrasonography includes a separate mention of ‘post treatment changes’ comprising of imaging features seen routinely on follow up examinations,
such as ‘ scar site seromas’ ,
fat necrosis ,
dystrophic calcifications etc.
Recognition of these features and a clear communication of these findings with the treating clinician is of utmost importance to avoid unnecessary interventions and facilitate appropriate patient management.
UPDATES IN THE MRI LEXICON
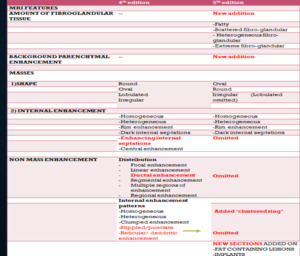
Fig. 10: The table reveals important modifications made to the MRI lexicon in the 5th edition of BIRADS.
Contrast-enhanced breast MRI has proven to be an imaging modality for the detection of breast cancer with highest sensitivity.
Though it has found widespread use in clinical practice,
standardisation of breast MRI techniques and protocols among different facilities and institutions is lacking which leads to discrepancies in image interpretation.
The updated BI-RADS fifth edition has attempted to address this problem in its new section on technique which encompasses recommendations for imaging acquisitions and sequences,
using a dedicated breast coil,
and contrast administration to obtain high-quality breast MRI images for accurate interpretation.
AMOUNT OF FIBRO GLANDULAR TISSUE AND BACKGROUND ENHANCEMENT
- The BIRADS lexicon incorporates 4 terms that describe the amount of BPE: “minimal”,
“mild”,
“moderate”,
and “marked”.
Though BPE does not correlate with the fibro-glandular parenchyma on mammography,
it does depend on the amount of fibro-glandular tissue present.
- Furthermore,
quantifying the level of enhancement is important as the sensitivity of detecting malignancy has been found to decrease,
as the level of background parenchymal enhancement increases.
Thus,
it may impair the diagnostic accuracy of the examination; and must be taken into account by the treating physician.
[6]
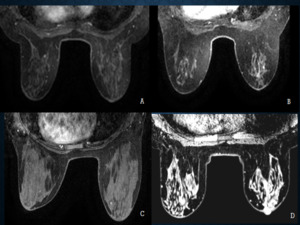
Fig. 11: Types of background enhancement, is a new descriptor added to the BIRADS lexicon. Figure ‘A’ reveals minimal background enhancement, ‘B’ reveals ‘mild’ enhancement, ‘C’ reveals moderate enhancement and ‘D’ reveals marked background enhancement.
MASS
DESCRIPTION
SHAPE: ‘‘Lobular’’ as a descriptor has been removed from the MRI section since lobulated masses are now included under the descriptor of ‘‘oval’’.
This helps align the description with the terminology utilized in other modalities,
such as mammography and ultrasound.
PATTERN OF ENHANCEMENT:
Due to under-utilisation,
descriptors such as “central enhancement”,
and “enhancing internal septations” for masess as well as “reticular” and “dendritic” for non-mass enhancement have been removed.
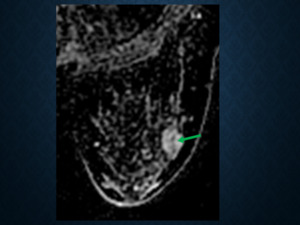
Fig. 12: Dark non enhancing septae (green arrow) in a fibroadenoma. The terminology of ‘enhancing septae’ has been omitted.
The term “ductal” enhancement,
is considered synonymous with the pattern of “linear” enhancement and has thus been eliminated.
Terminologies such as “multiple foci” and “stippled” patterns,
are now considered to represent normal enhancement of fibro-glandular tissue and have thus been omitted.
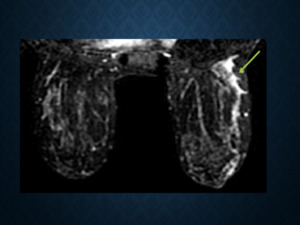
Fig. 13: The term ‘ductal enhancement’ has been omitted, as it is synonymous with the ‘linear enhancement’ pattern (green arrow).
A new terminology to describe non-mass enhancement that has been introduced into the MRI lexicon,
“clustered ring enhancement”,
which denotes suspicious enhancement of periductal stroma and has been shown to have a high positive predictive value (PPV) for ductal carcinoma in situ.
Thus,
recognition of this pattern is associated with a high index of suspicion for malignancy.
[7]
NEW SECTION ON FAT CONTAINING LESIONS
The section on fat-containing lesions essentially pertains to benign findings such as fat necrosis,
lymph nodes with maintained fatty hila,
hamartomas,
post-operative changes with fat content such as hematomas with fat.
However,
careful evaluation of certain lesions is warranted,
such as lymph nodes with preserved fatty hila could still be suspicious,
and some malignancies could demonstrate internal fat.
NEW SECTION ON IMPLANTS
MRI is undoubtedly the best imaging modality for evaluation of implant integrity and is often helpful in cases that are equivocal on mammography or ultrasonography.
MRI is the most appropriate for evaluation of silicone implants,
with a sensitivity of 72-94% for silicone implant rupture evaluation and a specificity of 85%-100%,
making it superior to mammography and sonography.
The new section on breast implants,
describes the implant type,
location,
and imaging findings commonly seen in intact and ruptured implants.
The descriptors for intracapsular rupture such as ‘radial folds’,
‘subcapsular line’,
‘keyhole sign,’ and ‘linguini sign’ have been added,
thus meticulous assessment to specifically look for these findings becomes imperative.
On similar lines,
subtle findings such as ‘a focal bulge’ along the implant must be recognized and reported by the radiologist to draw attention to a possible focal weakening of the implant capsule,
which may later lead to a rupture hence requiring follow up examinations.
[6]
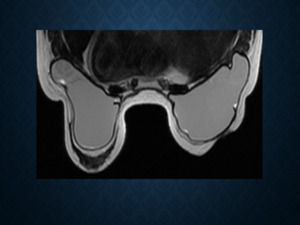
Fig. 14: A new section on ‘Implants’ has been added which includes a description of the implant type, location, and imaging features of intact and ruptured implants.
Changes to assessment categories in the BI-RADS fifth edition
One of the major changes in the new BI-RADS edition has also been the de-linking of assessment categories and management recommendations.
Though,
the assessment and management have been paired up appropriately in majority of the cases,
there are some instances where the management recommendations may not correlate with the BI-RADS assessment,
for example,
a benign finding may require image guided intervention or surgical management.
This may occur when a patient presents with a palpable mass without suspicious imaging findings,
still requiring surgical management,
or cases of breast abscesses where drainage may be necessary,
or even therapeutic cyst aspirations due to patient discomfort.
The new edition thus provides flexibility for discordances between the assessment and the management [1]
