ECR 2018 / C-2086
A Guide to the Sonography of the Eye and its Role in Ophthalmological Emergencies.
Congress:
ECR 2018
Poster Number:
C-2086
Type:
Educational Exhibit
Keywords:
Education and training, Diagnostic procedure, Ultrasound-Colour Doppler, Ultrasound, Eyes, Emergency, Anatomy
Authors:
D. Solís Gutiérrez1, R. Navas1, E. Alvarez2, R. Ortiz1, I. Ariño1; 1Zaragoza/ES, 2Soria/ES
DOI:
10.1594/ecr2018/C-2086

Fig. 3:
Standard Ultrasound machine equipped with realtime high-frequency probe.

Fig. 4:
US technique. Standard examination showing the
position of the transducer to...

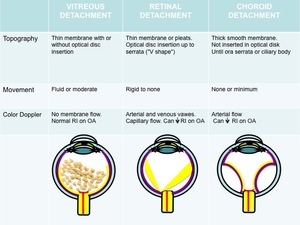
Table 1:
Differential diagnosis of the posterior segment detachments.

Fig. 5:
Pulsed Doppler ultrasound of the ophthalmic artery shows normal wave and...

Fig. 6:
Acute vitreous hemorrhage with posterior hyaloid detachment in post-traumatic...

Fig. 7:
Posterior vitreous detachment. Fine floating echoes and more heterogeneously...
.")
Fig. 8:
Subretinal haemorrhage. Retinal detachment with subretinal space filled with...

Fig. 9:
Acute Retinal detachment and vitreous hemorrhage. Echogenic mobile lines with...

Fig. 10:
Tractional retinal detachment in patient with vision loss and history of...

Fig. 11:
US Colour Doppler scan showing an acute Rhegmatogenous retinal detachment.

Fig. 12:
Choroidal detachment. Convex and peripheral white line, separating from the...

Fig. 13:
Choroidal detachment. Two lines ballooning into the vitreous.

Fig. 14:
Color Doppler US shows vascular echogenic membranes demonstrating choroidal and...

Fig. 15:
Choroidal melanoma. Posterior wall mass with choroidal excavation and vitreous...
.")
Fig. 16:
Choroidal melanoma. Endophytic growth into the vitreous chamber with vitreous...

Fig. 17:
Melanoma of ciliary body. B-mode US.

Fig. 18:
Choroidal metastases. Colon adenocarcinoma.

Fig. 19:
Choroidal metastases. Colon adenocarcinoma.
Color Doppler US shows irregular...