Introduction
Acute scrotal pain in adults is a common urological emergency requiring fast diagnosis and treatment.
Although the majority of patients with acute scrotal pain are usually young adults,
any age group can be affected.
The right diagnosis is crucial and leads to the decision of a conservative or surgical treatment.
Acute scrotum is a challenging clinical problem.
Correct diagnosis is crucial to determine appropriate treatment.
Anatomy
The anatomic structures that may be involved in the pathology of scrotum are the testis,
tunica vaginalis,
epididymis,
spermatic cord,
appendix testis,
appendix epididymis and other appendix structures (Fig.
1).
Testicular size depends on age and stage of sexual development.
In the postpubertal male the testes measure approximately 5 x 3 x 2 cm [1].
The fibrous tunica albuginea covers the testis.
The tunica albuginea is covered by the tunica vaginalis,
except at the points of attachment of the epididymis to the testis,
and along its posterior border,
where the spermatic vessels enter the gland.
The epididymis is located superior to and adjacent with the posterior aspect of the testis.
Four testicular appendages have been described: the appendix testis,
the appendix epididymis,
the vas aberrans and the paradidymis.
These are remnants of embryonic ducts [2].
The appendix testis and the appendix epididymis are usually seen at scrotal US [1].
The spermatic cord starts at the deep inguinal ring and descends vertically into the scrotum.
It is composed by the vas deferens,
testicular artery,
cremasteric artery,
deferential artery,
pampiniform plexuses,
genitofemoral nerve and lymphatic vessels [3,
4].
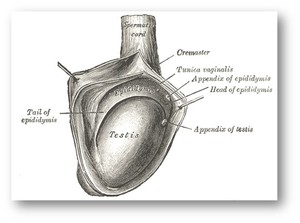
Fig. 1: The anatomic structures that may be involved in the pathology of scrotum are the testis, tunica vaginalis, epididymis, spermatic cord, appendix testis, appendix epididymis and other appendix structures.
References: Gray, Henry 1918. Anatomy of the Human Body. Revised by Warren H. Lewis.
US Anatomy
The normal scrotal wall thickness is approximately 2–8 mm [1].
Pubertal and postpubertal testes are of medium homogeneous echogenicity (Fig.
2).
The tunica albuginea can be seen as a thin echogenic line around the testis.
The space between the two layers of the tunica vaginalis normally contains small amounts of fluid,
seen as a thin echo-free line (Fig.
2).
This is a normal amount of fluid and it should not be misinterpreted as hydrocele [1].
The epididymis is best evaluated in a longitudinal view.
The head of the epididymis is depicted as a pyramidal structure 5–12 mm adjacent to the superior pole of the testis.
It is usually isoechoic to the testis.
The body of the epididymis,
when normal,
is usually indistinguishable from the surrounding peritesticular tissue and it measures 2–4 mm.
The tail of the epididymis is 2–5 mm in diameter and can be seen as a curved structure at the inferior pole of the testis [1].
The normal appendages,
appendix testis and appendix epididymis,
are typically seen only when a hydrocele is present.
The appendix testis appears as an ovoid structure 5 mm in length [1].
It is usually isoechoic to the testis but it can also be cystic.
The appendix epididymis is more often pedunculated [1] (Fig.
3).

Fig. 2: Normal testicular anatomy: a) axial and b) longitudinal plane of the testis. The double layered tunica vaginalis (white arrows) surrounds the testis. The tunica albuginea is not easily seen and is covered by the deep layer of the tunica vaginalis.

Fig. 3: Normal testicular appendages. a) appendix testis with calcifications, b)
appendix testis, c) cystic appendix epididymis.


 axial and b) longitudinal plane of the testis. The double layered tunica vaginalis (white arrows) surrounds the testis. The tunica albuginea is not easily seen and is covered by the deep layer of the tunica vaginalis.")
 appendix testis with calcifications, b)
appendix testis, c) cystic appendix epididymis.")