US has an important role in the diagnosis of acute scrotum in the emergency department.
Scrotal US is performed with the patient lying in a supine position.
A 6-15 MHz high-frequency linear-array transducer is used.
The testes are evaluated in longitudinal and transverse planes.
It is always important to compare the size and echogenicity of each testis and epididymis.
In patients being evaluated for an acute scrotum,
the asymptomatic side should be examined primarily in order to set the gray-scale and color Doppler gain settings to allow comparison with the affected side.
The use of color and power Doppler is mandatory to evaluate blood flow in the testis and in the epididymis,
as well as in the surrounding scrotal structures.
In equivocal cases,
CEUS is used to elucidate uncertain findings.
In our department CEUS is carried out immediately after US when a definite diagnosis cannot be reached.
A bolus injection of 4.8 mL SonoVue (BR1; Bracco,
Milan,
Italy) is performed through a 20-gauge cannula in the forearm,
followed by 10 mL normal saline (0.9%).
The power of the US beam (Mechanical Index MI) is set at the minimum and the focus placed at the end of the field of view to obtain the minimum of microbubbles destruction.
SonoVue is entirely an intravascular agent so it does not elude into surrounding tissue resulting to a true vascularization to the observed area.
This is very important when we want to access tissue viability.
Differential diagnosis of the commonest pathologic conditions includes testicular torsion,
torsion of testicular/epididymal appendix,
epididymitis,
epididymo- orchitis,
testicular trauma,
thrombosis of varicocele,
testicular abscess,
testicular tumor,
spermatocele,
and inguinal hernia.
Testicular torsion
Testicular torsion is a urologic emergency and it can occur at any age [5]. US plays an important role in differentiation between acute epididymo-orchitis from testicular torsion,
which demands surgical treatment.
In testicular torsion,
venous obstruction occurs first,
followed by arterial obstruction and eventually to testicular ischemia. A nearly 100% salvage rate exists within the first 6 hours after the onset of symptoms,
a 70%,
within 6–12 hours, and a 20% rate within 12–24 hours [1].
If access to scrotal US is unavailable or if US cannot exclude testicular torsion,
surgical exploration is recommended [6].
Key findings:
B mode US:
• Enlarged testis
• Normal or decreased echogenicity of the testis
• Enlargement of the epididymis
• Reactive hydrocele,
• Thickening of scrotal skin
Color Doppler:
• Complete (>360 degrees): Absence of intratesticular flow (Fig.
4),
• Incomplete (<360 degrees): Decreased intratesticular flow & elevated RI.
CEUS:
• Absence of contrast enhancement of testis in complete torsion and partial absence of enhancement in incomplete torsion (Fig.
5).
In the case of partial torsion a potential advantage of CEUS can be assumed.
According to only a few cases reported in the literature,
the only signs suggested for this difficult diagnosis are the asymmetry in the spectral flow between the testes or the absence of positive diastolic flow on pulse wave Doppler [1].
Since CEUS is able to reveal the venous flow of the testis,
it may be able to reveal venous engorgement,
not detectable with color Doppler,
offering the chance to identify incomplete testicular torsion.
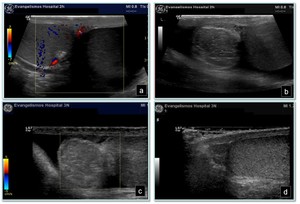
Fig. 4: Testicular torsion: a) color Doppler reveals no vascularization in the left testis which is hypoechoic relative to the right testis, b) enlarged left epididymis and moderate hydrocele, c) color Doppler shows no flow in the left epididymis, d) normal right testis and epididymis.

Fig. 5: Acute torsion: a) color Doppler showing normal vascularization of the right testis, b) color Doppler showing no vascularization of the left testis, (c, d) after contrast agent administration the absence of enhancement in the left testicle is clear. Due to absolute absence of testicular blood flow and complete lack of contrast medium the left testis appears totally dark
Torsion of the appendix testis
These cases are managed conservatively. The pain usually resolves in 2–3 days,
with atrophy of the appendix,
which may calcify.
The role of US examination in torsion of testicular appendages is to exclude testicular torsion and acute epididymo-orchitis.
Key findings:
B mode US:
• Hyperechoic mass with a central hypoechoic area adjacent to the testis or epididymis [7]
• Reactive hydrocele
• Skin thickening
Color Doppler:
• Increased peripheral flow may be seen around the twisted testicular appendage
• Normal vascularity of the testis at color Doppler.
CEUS:
• Normal enhancement of the testis
A spherical shape and size of 6 mm with no internal vascularity and peripherial vascularity on Doppler scan are highly suggestive of torsion [8].
Segmental testicular infarction
Segmental testicular infarctions usually result from arterial embolization or thrombosis.
The main causes of a segmental testicular infarct include orchitis,
sickle cell disease,
trauma,
vasculitis and pelvic surgery.
Segmental testicular infarction usually presents with testicular pain and is often indistinguishable at US from testicular malignancy.
Key findings:
B mode US:
• Focal hypoechoic region in the testis
• Wedge-shaped or rounded
Color Doppler:
• Absence of color Doppler flow in the hypoechoic region.
CEUS:
• Avascular or hypovascular lesion with intralesional flow
In the cases of testicular infarction CEUS allows a more confident diagnosis of segmental infarction,
compared to grey-scale and color Doppler.
However the differential diagnosis with hypovascular testicular tumor may be problematic based on imaging alone,
especially if the lesion is rounded [9] (Fig.
6).

Fig. 6: Segmental testicular infarction: a, b) color Doppler showing absence of flow in the hypoechoic regions of the testis, c) B-Mode US shows a sharp heterogeneous testicle echostructure, d) CEUS showing focal absence of enhancement, consistent with segmental infarctions.
Orchitis
Orchitis is rarely isolated.
Almost all cases it is associated with epididymitis.
Isolated orchitis can be seen in mumps and syphilis.
In cases of orchitis hyperemia and heterogeneity isolated to the testis can be seen.
In normal testes detecting intratesticular venous flow is difficult.
Thus,
increased,
easily detected venous flow is highly suggestive of orchitis [9,
10] (Fig.
7-8).
Key findings:
B mode US:
• Hypoechogenicity: focal or diffuse
• Enlarged testis
• Scrotal wall thickening
• Hydrocele in the ipsilateral scrotum.
Color Doppler:
• increased vascularity
CEUS:
• Increased vascularity of testis

Fig. 7: Right sided scrotal pain-orchitis: a) hypervascularity and b) enlargement of the right testis (R) in comparison to the left (L) testis.

Fig. 8: Left sided scrotal pain-orchitis: US shows a sharp heterogeneous echostructure of the left testis.
Epididymitis
Epididymitis (Fig.
9) may be associated with inflammation extending to the testis,
(epididymo-orchitis).
Epididymo-orchitis and epididymitis are common causes of acute scrotal pain in adolescent boys and adults.
Clinically,
scrotal pain associated with epididymitis is usually relieved when the testes are elevated over the symphysis pubis (the Prehn sign) [11].
Negative Prehn sign points towards testicular torsion which is a surgical emergency.
Key findings:
B mode US:
• Enlarged hypoechoic epididymis
• Reactive hydrocele or pyocele
• Scrotal wall thickening
Color Doppler:
• Increased vascularity
CEUS:
• Increased vascularity of epididymis
• Normal enhancement of the testis

Fig. 9: Acute Epididymitis-different pattients: a, b) swelling and increased vascularity in the epididymeal tail with normal testicular blood flow, typical of inflammation.
The epididymis is the organ primarily involved in epididymo-orchitis,
with orchitis developing in 20–40% of cases due to direct spread of infection.
Testicular involvement is confirmed by the presence of testicular enlargement and inhomogeneous testicular echotexture [12] (fig.
10).

Fig. 10: 65 year old male patient one month after treatment – Subacute epididymo-orchitis and spermatic cord inflammation:
a) US showing heterogeneity of the left testis and scrotal wall thickening,� b) color Doppler showing decreased vascularization of the testis c) color Doppler showing enlarged hypervascular right epididymis, d) Slightly increased vascularization of the spermatic cord.
Epididymal / Testicular abscess
Epididymal (Fig.
11) or testicular abscess is a complication of acute epididymitis or epididymo-orchitis.
Testicular abscess can also result from bacterial infection in an existing hematoma (as a result of testicular trauma) or in an infarction (secondary to testicular torsion or mumps) [13].
Key findings:
B mode US:
• Hypoechoic lesion with hypervascular margins in the testis or epididymis
• Scrotal wall thickening
Color Doppler:
• Focal avascular region with surrounding increased vascularity
CEUS:
• Hypoechoic lesion with peripheral rim of enhancement

Fig. 11: Epididymitis with abscess formation: color Doppler reveals a nonvascular hypoechoic area (abscess) surrounded by a hypervascular epididymis.
Scrotal trauma
Testicular trauma is the third most common cause of acute scrotal pain [14].
US is the imaging modality of choice,
allowing reliable identification of testicular and extratesticular injuries.
CEUS is useful to evaluate testicular trauma because of its capacity to demonstrate parenchymal vascularization.
It reveals fracture lines and intratesticular hematoma,
interruption of the tunica albuginea and extratesticular hematoma.
Key findings:
B mode US:
• Heterogeneous testis or testis absent from scrotum in case of dislocation
• Hematocele
• Disruption of tunica albuginea in case of testicular rupture (Fig 12)
• Scrotal wall hematoma
• Enlarged heterogenous epididymis or fragmented epididymis
• Mass with variable echogenicity located superior to the testis in case of spermatic cord hematoma
Color Doppler:
• loss of vascularity in the affected/ruptured portion of the testis or epididymis
• Yin Yang sign and to-and fro-flow pattern in case of pseudoaneurysm formation
CEUS:
• Hypoechoic interruption of the border of the testis with microbubbles within hematoma in case of testicular rupture with active bleeding

Fig. 12: Traumatic testicular rupture: a, b) hypoechoic components with little flow representing small contusions/hematomas, c, d) large disruption of tunica albuginea (arrows), e) hematocele.
Testicular Tumor
Testicular tumors usually emerge in young patients as a painless increase in the testis size accidentally noticed by the patient.
10% of testicular tumors present acutely with pain,
swelling or inflammation,
thought due to hemorrhage or infiltration [15].
The most common tumor to present with acute scrotum is seminoma.
Seminoma infiltrates the seminiferous tubules causing obstruction [16].
Lymphomas constitute 5% of testicular tumors and are almost exclusively diffuse non-Hodgkin lymphoma B-cell tumors [17].
Involvement of the spermatic cord and epididymis suggests lymphoma more than seminoma (Fig.
13).
Key findings:
B mode US:
• Focal lesion with increased vascularity at color Doppler
• Rounded,
circumscribed mass which displaces intra-testicular vessels (focal orchitis is usually peripherally placed and crescent in shape)
Color Doppler:
• Focal lesion with increased vascularity
CEUS:
• Focal lesion with increased enhancement in early phase and rapid wash-out

Fig. 13: Testicular lymphoma: a) B-mode US demonstrates a focal hypoechoic lesion in the lower pole of the testis, b) on CEUS, particulate movement of contrast (arrows) is seen throughout the lesion in a haphazard pattern, which confirms the presence of vascularity within the lesion. The final diagnosis was testicular lymphoma.
Varicocele
The veins of the pampiniform plexus normally range from 0.5 to 1.5 mm in diameter,
with the main draining vein being as large as 2 mm in diameter.
Varicoceles are more common on the left side (Fig.
14).
Key findings:
B mode US:
• Multiple,
hypoechoic,
serpiginous,
tubular structures of varying sizes larger than 2 mm in diameter
Color Doppler:
• Low-flow velocities help confirm the venous flow pattern,
with phasic variation and retrograde filling during a Valsalva maneuver

Fig. 14: 14: male in early 30s with a dull left scrotal pain-varicocele: a, b) dilated venous plexus-moderate varicocele.
Varicocele thrombosis
Spontaneous thrombosis of the pampiniform plexus (Fig.
15) is very uncommon.
Patients may present with acute scrotal pain mimicking a testicular torsion or strangulated hernia.
Key findings:
B mode US:
• Varicocele with echogenic debris within the dilated veins
Color Doppler:
• Absent or diminished flow within the dilated veins.
CEUS:
• Absent or diminished enhancement within the dilated veins.

Fig. 15: Varicocele thrombosis: US demonstrates normal testicles. a) color Doppler of the spermatic cord: enlarged spermatic vein without Doppler signal, b) there is a moderate sized left varicocele with echogenic debris demonstrated within the dilated veins. Color Doppler flow is significantly diminished and increased minimally with the Valsalva manoeuvre, c) US showing the dilated thrombosed veins as well as a hydrocele with internal echoes
Spermatocele
Spermatocele (Fig.
16) is a cystic dilatation of tubules of the efferent ductules in the head of the epididymis.
It usually is a painless,
incidental finding but can present as a mass lesion if it is large in size.
Key findings:
B mode US:
• Well-defined epididymal hypoechoic lesions usually measuring 1-2 cm
• Usually irregular,
with fine low-level internal echoes and sometimes septations.
Color Doppler:
• Absence of color Doppler flow
CEUS:
• No enhancement

Fig. 16: Spermatocele. US reveals a cystic lesion with fine low-level internal echoes and septations in the head of the epididymis.
Rete Epididymis
Rete epididymis or tubular ectasia of the epididymis (Fig.
17) typically occurs in patients with prior vasectomy.
It can be also seen with other causes of obstruction of the ductus deferens.
Key findings:
B mode US:
• Enlargement of the epididymis with diffuse finely speckled appearance
Color Doppler:
• Absence of color Doppler flow

Fig. 17: Rete Epididymis (tubular ectasia of the epididymis): US shows mild enlargement of the epididymis with multiple cystic interfaces-speckled appearance.
Fournier Gangrene
Fournier gangrene (Fig.
18) is a polymicrobial necrotizing fasciitis of
the scrotum that frequently extends to the lower abdominal wall.
It constitutes a urologic emergency for which early recognition is demanded.
US hallmark of Fournier gangrene is subcutaneous gas within the scrotal wall [1].
Key findings:
B mode US:
• Numerous,
discrete,
hyperechoic foci with reverberation artifacts in the scrotal wall (air)
• Scrotal wall thickening
• Testes and epididymides are normal (due to their separate blood supply)
Color Doppler:
• The scrotal wall shows increased vascularity

Fig. 18: Fournier Gangrene: a) US shows scrotal wall edema and dirty shadowing due to gas foci, b) US shows edematous thickened scrotal wall with pus pockets and air in the scrotal wall, c) color Doppler reveals the testicles with normal vascularity.
Inguinal- scrotal hernia
Inguinal–scrotal hernia (Fig.
19) usually present as a palpable mass with indolent aching pain and less frequently as acute scrotal pain and swelling.
The presence of bowel loops or omental fat within the scrotum identify the occurrence of a hernia.
Key findings:
B mode US:
• Bowel loop or omental fat within the scrotum.
The presence of real-time peristalsis is diagnostic for the presence of bowel
Color Doppler:
• Hyperemia of scrotal soft tissues could be a sign of incarceration

Fig. 19: Inguinal-scrotal hernia: presence of fluid filled bowel loops and omental fat in the scrotum.
Acute idiopathic scrotal edema
Acute idiopathic edema (Fig.
20) occurs rarely in adults [18].
Infection and angio-edema are suggested as possible causes.
It clinically presents with unilateral pain,
swelling and erythema.
It resolutes automatically within three days.
Key findings:
B mode US:
• Scrotal wall thickening and edema
Color Doppler:
• Hyperemia of the scrotal wall.

Fig. 20: Acute unilateral scrotal edema: the scrotal wall (white arrow) measures 3.5 cm in width and the testis (red arrow) is depicted approximately 7 cm from the scrotal skin in depth.

 measures 3.5 cm in width and the testis (red arrow) is depicted approximately 7 cm from the scrotal skin in depth.")

 color Doppler reveals no vascularization in the left testis which is hypoechoic relative to the right testis, b) enlarged left epididymis and moderate hydrocele, c) color Doppler shows no flow in the left epididymis, d) normal right testis and epididymis.")