ECR 2018 / C-2210
Thoracic metastases: a pictural review.
Congress:
ECR 2018
Poster Number:
C-2210
Type:
Educational Exhibit
Keywords:
Cancer, Diagnostic procedure, CT, Thorax, Mediastinum, Lung
Authors:
I. Ben Amara1, S. Esseghaier2, R. Aouini3, M. CHAABOUNI3, N. REGAYA4, A. Zidi3; 1Tunis, tunis/TN, 2menzah 7/TN, 3Tunis/TN, 4megrine/TN
DOI:
10.1594/ecr2018/C-2210

Fig. 1:
Pulmonary metastases: typical pattern of solid nodules.
CT of a patient with...
.
References: Salah Azaiez institute, Tunis/ Tunisia")
Fig. 2:
Pulmonary metastases: atypical pattern of solid nodules
CT of a patient with...

Fig. 3:
Pulmonary metastases: typical cavitary nodules
CT of a patient with an...

References: Salah Azaiez institute, Tunis/ Tunisia")
Fig. 4:
Pulmonary metastases: Typical cavitary nodule
CT of a patient with a rectal...

Fig. 5:
Pulmonary calcified metastases from femoral osteosarcoma in a 9 years old...

Fig. 6:
Pulmonary calcified metastases from osteosarcoma
CT shows right calcified...

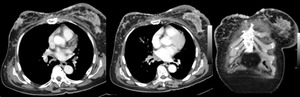
Fig. 8:
Endobronchial metastases from breast cancer. CT shows bronchial wall thickening...

Fig. 7:
Endobronchial metastases from rectal adenocarcinoma. CT shows soft tissue...

Fig. 9:
Lymphangitic carcinomatosis from gastric adenocarinoma.
Chest X ray shows...

Fig. 10:
Lymphangitic carcinomatosis from breast cancer. CT shows diffuse nodular...

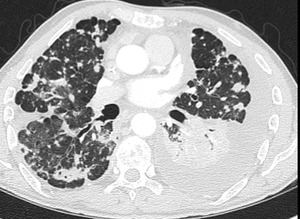
Fig. 11:
Lymphangitic carcinomatosis from pancreatic adenocarcinoma.
CT shows diffuse...

Fig. 12:
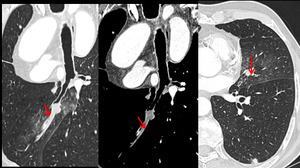
Endovascular metastases:
CT shows tumoral invasion of pulmonary right artery...

Fig. 13:
Metastatic mediastinal lymphadenopathy
CT scan shows enlarged mediastinal...

Fig. 14:
Pleural metastases from ankle synovialosarcoma. Chest X ray and CT show...

Fig. 15:
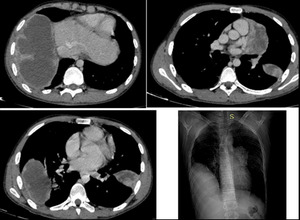
Cardiac metastases from osteosarcoma.
CT scan shows calcified masses involving...

Fig. 16:
Cardiac metastases:
CT scan shows myocardial masses involving the...

Fig. 17:
Cardiac metastases
Cardiac magnetic resonance imaging shows multiple masses...
 and nodular pericardial thickening (red arrow); It also shows right pleural effusion (blue arrows).
References: Salah Azaiez institute, Tunis/ Tunisia")
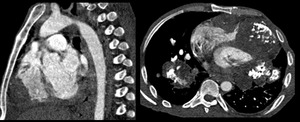
Fig. 18:
Cardiac metastases from breast cancer.
CT shows voluminous mass within the...
.
References: Salah Azaiez institute, Tunis/ Tunisia")
Fig. 19:
Metastatic pericardial effusion from breast cancer
CT shows large global...

Fig. 20:
Bone metastasis from breast cancer
CT shows unique vertebral sclerotic...

Fig. 21:
Bone metastases from breast cancer
CT shows diffuse bone metastases

Fig. 22:
Cutaneous and subcutaneous metastases in a patient with breast cancer