Due to its depth,
ultrasound is often of limited use for retroperitoneal evaluation.
Computed tomography (CT) and magnetic resonance (MR) play a key role in the assessment of retroperitoneal masses.
Familiarity with the spectrum of CT and MR findings in the different diseases would help for accurate diagnosis.
NON-NEOPLASTIC LESIONS
RETROPERITONEAL FIBROSIS
*Author's note: Although there are forms of malignant retroperitoneal fibrosis,
for educational and clarity purposes,
retroperitoneal fibrosis is classified as non-neoplastic taking into account that the idiopathic and benign forms make up the vast majority of cases.
Retroperitoneal fibrosis includes a wide range of diseases characterized by the proliferation of fibroinflammatory tissue around the aorta,
inferior vena cava,
and iliac vessels.
In approximately 70% of cases,
it is idiopathic.
♦ IDIOPATHIC RETROPERITONEAL FIBROSIS
Idiopathic retroperitoneal fibrosis (RPF) is a rare disease .
Its pathogenesis is still unknown although,
given that atherosclerosis is frequent among patients with RPF,
it is considered to be an excessive local inflammatory response to Ag presents in the atherosclerotic plaques of the abdominal aorta.
Other authors contemplate it as a systemic affectation of autoimmune origin rather than a local one considering its frequent association with many other systemic autoimmune diseases.
Sometimes,
it appears as part of the IgG4-related disease or multifocal fibrosclerosis.
The diagnosis of RPF is a challenge for clinicians because it presents with nonspecific symptoms.
When it progresses,
the symptoms are related to the compression or entrapment of the neighboring structures:
-
Ureters: obstructive uropathy,
renal failure…
-
Retroperitoneal venous and lymphatic structures: lower limb edema,
deep vein thrombosis.
-
Much less frequently,
there are described cases of compression of the colon causing constipation,
or of the aorta or iliac vessels causing claudication
Radiological findings:
-
CT is useful for the diagnosis,
as well as the assessment of the affectation of neighboring organs,
the detection of frequently associated conditions and the follow-up.
It appears as a well-defined,
irregular soft tissue mass that may infiltrate adjacent organs.
Usually,
it does not affect the retroaortic space and does not cause aorta displacement.
The enhancement varies according to the phase,
being avid in the early phases,
and practically absent in late inactive phases when fibrosis predominates (Fig. 4).
Treatment is based predominantly on medical strategies consisting of corticosteroids,
immunosuppressants or tamoxifen.
Drainage of the upper urinary tract with nephrostomy tubes may be necessary in case of periureteral involvement which is very frequent in the idiopathic form.
Surgery is reserved only for refractory cases.
♦ SECONDARY RETROPERITONEAL FIBROSIS
Secondary retroperitoneal fibrosis constitutes a third of cases.
Several causes have been described as shown in Table 2.
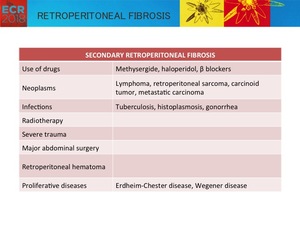
Table 2: Causes of secondary retroperitoneal fibrosis
Benign forms,
as well as the idiopathic form,
usually have a good prognosis if promptly diagnosed and adequately treated.
Malignant forms,
usually secondary to metastatic retroperitoneal involvement or a primary retroperitoneal tumor,
are the most relevant due to its poor prognosis.
As adequate treatment depends on the cause,
the distinction between benign and malignant causes becomes crucial.
Several findings have been proposed as suggestive of malignancy as it is shown in the table below (Table 3).
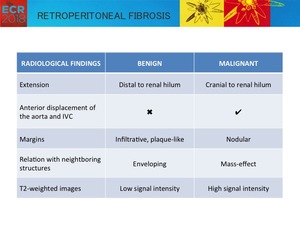
Table 3: Radiological findings that may help differentiate benign from malignant RPF.
The sensitivity and specificity of these characteristics,
however,
is not sufficient to allow the differentiation between benign and malignant forms,
but they may help in the diagnosis of RPF.
IgG4-RELATED DISEASE
In 2003,
Kamisawa et al.
suggested the concept of IgG4-related disease to refer to a group of disorders with common pathologic,
serologic and clinical features.
Therefore,
it is a recently recognized entity,
characterized by the infiltration by IgG4-positive plasma cells in multiple organs,
which is often accompanied with elevated serum IgG4 concentrations.
As clinical symptoms are usually minor,
diagnosis is often incidental after organ swelling is identified at imaging.
The most commonly affected organ is the pancreas in the form of sclerosing autoimmune pancreatitis (Fig. 7,
image B).
However,
IgG4-related disease has been identified in a wide variety of extrapancreatic organs ( Table 4).
When it compromises the retroperitoneum,
the affection may include retroperitoneal fibrosis,
aortitis or aortic aneurysm.
Clinically nonspecific,
it may manifest as back pain or symptoms due to hydronephrosis secondary to ureteral entrapment.
Radiological findings:
On cross-sectional imaging,
a soft tissue mass is identified involving the infrarenal abdominal aorta and iliac vessels which can extend and trap both ureters leading to renal failure (Fig. 5).
IgG4-related periaortitis manifests as a thickening of the aortic wall surrounded by a non-stenotic mass with irregular margins.
Aneurysmal dilatation of the abdominal aorta may be associated,
and in some series,
up to 57% of aortic dilatations are considered to be associated with the IgG4-related disease.
The aberrant tissue presents homogeneous enhancement in the late phase of the contrast-enhanced CT .
At MRI,
signal intensity is variable depending on the degree of active inflammation (Fig. 6).
Response to steroid therapy is excellent in most patients (Fig. 8).
AORTITIS
It is a broad term to refer to inflammation of the aortic wall.
It has numerous causes,
classically classified as infectious and noninfectious,
which are distinguished by the pattern aortic involvement and the imaging findings.
CT and MRI are the most commonly used radiological tests,
with conventional angiography practically obsolete.
PET and ultrasound present limitations in the evaluation of morphologic changes the former and in the evaluation of the inflammatory activity the latter.
Therefore,
its use is limited to specific cases.
♦ NON-INFECTIOUS AORTITIS
Inflammatory involvement of the aortic wall is described in numerous rheumatic diseases,
among which are numerous vasculitis,
especially those that characteristically affect the great vessels (Takayasu arteritis and giant cell arteritis),
some spondyloarthropathies such as ankylosing spondylitis or seronegative spondyloarthropathies,
rheumatoid arthritis ...
Radiological findings:
In general,
the findings are limited to concentric thickening of the aortic wall.
Other findings that may be present according to the etiology are light stenosis,
complete lumen occlusion or aneurysm.
♦ INFECTIOUS AORTITIS
It is an inflammation of the aortic wall due to infection by microorganisms,
the most frequent being Staphylococcus aureus and different Salmonella species.
Without surgical history,
it is a very uncommon but life-threatening pathology.
There is greater susceptibility among men,
generally above 50 years of age and on abnormal aortic walls due to a predisposing pathology (Table 5).
The clinical presentation is nonspecific (fever,
pain,
elevated serum levels of acute phase reactants) therefore,
the diagnosis is frequently delayed.
Radiological findings:
- Thickening of the aortic wall
- Liquid or periaortic soft tissue mass,
with a variable extension that can raise the differential diagnosis with other periaortic lesions (retroperitoneal fibrosis,
periaortic hemorrhage,
lymphomatous tissue,
or adenopathies) ( Fig. 9).
- Saccular aneurysm or rapidly progressive pseudoaneurysm
- Exceptionally,
intramural gas bubbles
- Besides,
CT allows evidence of complications such as hydronephrosis,
abscesses,
aortoenteric fistulas or rupture.
-
In MRI: Although the evidence of radiological findings in MRI is meager, this technique allows an excellent assessment of the wall and lumen of the aorta,
being the technique of choice for serial follow-ups.
MRI findings are analogous to those on CT images.
MRI depicts a thickening of the aortic wall surrounded by periaortic abnormal tissue that appears typically hypointense on T1-weighted and hyperintense on T2-weighted images,
with homogeneous enhancement following the administration of contrast material ( Fig. 10 and Fig. 11).
RETROPERITONEAL HAEMATOMA
Retroperitoneal hemorrhage may be secondary to significant trauma,
anticoagulation therapy,
ruptured aneurysm or iatrogenic after surgical and interventional procedures.
Radiological findings:
The imaging findings vary according to the stage.
Acute or subacute hematomas have high attenuation at CT and may be hyperintense in T1 and T2-weighted images on MRI.
As it evolves,
its density decreases at CT,
and its signal intensity on MRI becomes low due to hemosiderin deposition.
RETROPERITONEAL AMYLOIDOSIS
Amyloidosis is a general term used to refer to a group of diverse diseases characterized by the extracellular deposition of a proteic material,
called amyloid.
Retroperitoneal involvement is rare and clinically may present as abdominal pain.
Radiological findings:
CT depicts a focal mass-like lesion,
which can infiltrate the retroperitoneum involving the abdominal aorta and its main branches.
Calcification is not uncommon over time.
NEOPLASTIC LESIONS
LYMPHOID AND HEMATOLOGIC NEOPLASMS
♦ LYMPHOMA
Primary retroperitoneal lymphoma
It is the most frequent primary retroperitoneal malignant tumor,
accounting for a third of the malignancies.
Radiological findings:
-
In CT,
it appears as a well-defined homogenous mass that extends infiltrating between tissues,
characteristically exerting little compression.
It can obstruct ureters,
causing ureterohydronephrosis,
and the inferior vena cava.
The anterior displacement of the aorta and the inferior vena cava is distinctive,
a sign known as a floating aorta.
After the administration of contrast,
it presents a moderate homogenous enhancement ( Fig. 12).
-
In the MRI,
it is isointense in the images weighted in T1 and iso or hyperintense in images weighted in T2 with homogenous enhancement ( Fig. 13).
When presented with patchy heterogeneous enhancement,
the difficult differential diagnosis with retroperitoneal sarcomatous tumors is considered.
The treatment consists of chemo and radiotherapy ( Fig. 14).
Renal lymphoma
Occasionally,
retroperitoneal lymphoid involvement is secondary to the transcapsular extension of renal disease.
The kidneys are the most common abdominal organ affected by lymphoma,
with estimation of renal involvement in 30-60% of patients according to autopsy series.
In up to 20% of cases,
the affection consists of a diffuse infiltration.
CT shows enlarged kidney (Fig. 15),
usually bilateral. The renal disease can extend through the renal capsule and invade the perirenal space.
This scenario is less frequent than a direct renal invasion from a contiguous bulky retroperitoneal mass.
♦ POST-TRANSPLANT LYMPHOPROLIFERATIVE DISEASE
Post-transplant lymphoproliferative disease occurs as a complication of a solid organ transplant and the consequent immunosuppression.
It is a proliferation of B lymphocytes which may manifest as an uncomplicated mononucleosis or a lymphoma.
Radiological findings:
On cross-sectional images,
it appears as adenopathies,
splenomegaly,
and masses affecting the liver and kidneys.
In the retroperitoneum,
a mass of soft tissues can be seen enveloping the aorta,
displacing it anteriorly.
♦ EXTRAMEDULLARY PLASMACYTOMA
Extramedullary plasmacytoma (EMP) is a monoclonal neoplastic proliferation of plasma cells.
In most cases it occurs in the aerodigestive tract; however,
any organ can be affected.
Radiological findings:
Retroperitoneal EMP usually affects the perirenal region as an extensive infiltrative soft-tissue mass,
with homogeneous contrast enhancement.
RETROPERITONEAL DISSEMINATION IN SIGNET RING CELL CARCINOMA
Signet ring cell carcinoma is a rare form of adenocarcinoma of aggressive clinical course and poor prognosis,
which is histologically characterized by cells with high intracytoplasmic mucin content that pushes the nucleus to the periphery.
Up to 96% arise from the stomach,
while the rest can originate from different organs: colon,
rectum,
gallbladder,
pancreas,
urinary tract and breast.
The determination of the primary source of the carcinoma is based on immunohistochemical profiles (expression of different cytokeratins).
However,
sometimes the profile is not specific.
Retroperitoneal involvement can occur by direct tumor infiltration or metastatic disease.
Radiology findings:
The best diagnostic technique is computed tomography.
CT shows a fibrotic soft-tissue mass,
infiltrating the retroperitoneum and enveloping the retroperitoneal structures ( Fig. 16).
Biopsy and histopathological analysis are usually necessary for accurate diagnosis.
The accurate evaluation of disseminated retroperitoneal disease is,
in any case,
of high importance,
as sometimes it dismisses the possibility of surgical treatment.
NEUROGENIC TUMORS
♦ MALIGNANT PERIPHERAL NERVE SHEATH TUMOR (MPNST)
Formerly known as neurofibrosarcoma,
it is a highly aggressive infiltrative tumor.
The most frequent location in the retroperitoneum is the paraspinal region.
Radiological findings:
Imaging techniques are not reliable when it comes to distinguishing it from its benign form.
However,
some features are suggestive of malignancy:



 Axial contrast-enhanced CT images show retroperitoneal soft-tissue mass (star) surrounding the great vessels and occupying the left perirenal space. B) Distal encasement of the left ureter and secondary hydronephrosis forced pig-tail catheter placement which can be seen in the left renal pelvis (arrow). Note the atrophy of the left kidney (arrowhead) which was secondary to chronic obstruction.")

 Contrast-enhanced CT scan shows an infiltrative hypoenhancing soft-tissue mass that covers the abdominal aorta (star), a finding that represents IgG4-related retroperitoneal fibrosis. Note that the mass spares the posterior aspect of the aorta. A and B) CT also shows slight enlargement of both kidneys produced by diffuse attenuation areas (arrows) due to IgG4-related renal disease.")
 Axial contrast-enhanced portal phase T1 weighted image and B) short tau inversion recovery (STIR) T2-weighted image shows a mild enhancing soft-tissue mass surrounding the abdominal aorta. C) The multiple bilateral renal focal lesions present intense restriction on axial DW image (B1000).")
 coronal contrast-enhanced CT image of the same patient performed a few months later shows a contrast-enhancing wall thickening of the common bile duct in its extrahepatic and intrapancreatic portions (arrow) with upstream dilatation, probably due to infiltration by IgG4-positive plasma cells. B) Axial CT image depicts discrete focal parenchymal enlargement of the pancreatic tail with loss of the normal lobular margin (arrowhead) as evidence of pancreatic involvement.")
 of the same patient shows clear reduction of pancreatic, retroperitoneal and renal lesions after steroid therapy.")

 Axial (A) anc coronal (B) contrast-enhanced CT images depicts a penetrating ulcer (arrowhead) in the wall of the infrarenal abdominal aorta surrounded by a periaortic extensive soft-tissue mass.")
 Axial fat-suppressed T1-weighted image shows irregularity of the aortic wall corresponding to penetrating ulcer (arrowhead) with loss of periaortic fatty planes. B) Axial T2-weighted image depicts periaortic heterogeneous collection. C) DWI and D) ADC map show restriction of the periaortic collection, compatible with active inflammation.")
 Coronal fat-suppressed contrast-enhanced T1-weighted image and B) T1- and color diffusion-weighted fusion image depict the penetrating ulcer (arrowhead) and the intense diffusion restriction of the periaortic collection.")

 Non-enhanced CT images show a hypoattenuating soft-tissue mass in the left perirenal space infiltrating the left renal hilum and extending superiorly to the ipsilateral adrenal gland. Axial (B) and coronal (C) enhanced CT images shows homogeneous enhancement of the infiltrative mass.")
 Axial contrast-enhanced portal phase T1 weighted imageshows an homogeneously enhancement of the soft-tissue mass infiltrating the perirenal space . C) B1000 diffusion-weighted image shows high restriction of the infiltrative mass and of multiple small right subcapsular lesions")
 after five cycles of chemotherapy shows significant size reduction of the retroperitoneal mass, currently circumscribed to the posterosuperior region of the left kidney.")
. Note also the retroperitoneal adenopathies.")
 Axial non-contrast CT depicts a soft tissue mass infiltrating both adrenal glands. B and C) Axial and D) coronal contrast-enhanced CT images show mild and homogeneus enhancement of the mass involving partially the right adrenal gland (arrow) and completely the left adrenal gland. The infiltrative tissue extends cranially over the renal vessels and inferiorly to the aortic bifurcation and the hilum of the kidney transplant in renal in the right lower quadrant (arrowhead).")
 Axial T1-weighted image and B) T2-weighted image shows a retroperitoneal mass. C) Axial portal phase contrast-enhanced MR image: The lesion shows scanty and delayed enhancement after administration of contrast, predominantly on the right side of the retroperitoneum (arrow). D and E) DW image and ADC map shows restriction of the infiltrative mass.
A biopsy was performed being positive for fragments of signet ring cell carcinoma. The inmunohistochemical analysis was not conclusive for primary origin. Unfortunately, the patient died and no further studies were carried out.")