|
What is Regional Analgesia ?
|
" Injection of local anaesthetic agent near a nerve or group of nerves in order to inhibit autonomic ,
motor or sensory (or all) impulse transmission through it"
Area affected depends upon where is Local Anaesthetic agent is injected along the nerve course .
the onset and duration of block depend upon both the type of nerve block and LA agent used .
| What is Mechanism of action of Local Anaesthetic ? |
LA agents work by binding to Sodium Channels located on nerve cell membranes rendering them inactive .
Inactive Sodium Channels can not participate in action potential generation leading to blockade of conduction of nerve impulse .
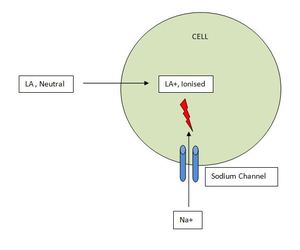
Fig. 1: Mechanism of Action of Local Anaesthetic Agents
Adjuvants are added to modify the duration and onset of analgesia by local aaesthetic agents.
Various adjuvants include epinephrine ,
Sodium bicarbonate,
Opioids,
Dexamethasone and Alpha2 agonists .
|
What are types of Regional Analgesia ?
|
Upper Extremity :-
- Interscalene Brachial Plexus Block
- Supraclavicular Brachial Plexus Block
- Infraclavicular Brachial plexus Block
- Axillary Block
- Wrist block
- Digital Nerve Block
Lower Extremity :-
- Lumbar plexus
- Femoral Nerve
- Fascia iliaca
- Obturator nerve
- Sciatic Nerve
- Popliteal nerve
- Saphenous nerve
- Ankle block
- Digital nerve Block
Head,
Neck and trunk :-
- Scalp block
- Cervical plexus
- Intercostal nerve
- Thoracic paravertebral
- TAS
- Ilioinguinal/Iliohyposgastric block
- Pudendal and Paracervical blocks
- Brachial Plexus Block
- Stellate ganglion block
- Phrenic Nerve Block
| Indications of Regional Analgesia in IR ? |
Common ones are -
For Vascular Procedures :-
- Endoluminal Laser ablation
- Angioplasty of lower limb
- Create percutaneous AV fistulas
- Uterine fibroid embolisation
For Non vascular Procedures :-
- RFA Hepatic tumors
- Percutaneous nephrolithotomy
- Peritoneal dialysis catheter placement
- Percutaneous lung FNAC
- Type 1 CRPS
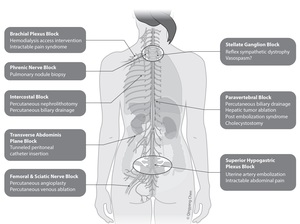
Fig. 2: Indications of Regional Analgesia/ Nerve Blocks in Various IR procedures
References: QC visuals ,Toronto
| Techniques of Nerve Localisation ? |
The nerve that is intended to be blocked can be localised by two broad ways -
Image Guidance - It can be by Ultrasound (Most Commonly used)
Flouroscopy
CT
Electric Stimulation
Here only Image guidance will be discussed
Ultrasound Guided Perpheral Nerve Block
Previuosly bony and surface landmarks were exclusively used to execute regional analgesia.However the efficacy and safety profile of PNB by this method is variable and most common cause for this is the inaccurate positioning of needle with respect to the target nerve.
Here Ultrasound comes to the rescue.
Ultrasound permits direct visualisation of the needle location relative to the target nerve,
blood vessels and the surrounding structures.
The placement of LA during and after injection can also be observed.
Technique
Usually high frequency probe (10-15 Mhz) is used to identify the superficial nerves (e.g upper limb) and lower frequency probe (5-7 Mhz) for deeper nerves (e.g sciatic nerve)
General steps for nerve block are discussed here and specific points with respect to important nerve blocks will be discussed later
Aftter sterile skin preparation ,
sterile probe and sterile gel is used to sonographically look for anatomicl structures at block site.
Target nerve,
blood vessels ,
bony and soft tissue structures are well identified .
Holding the probe immobile the needle is advanced & needle tip is continously visualised and tracked.
Hydrolocalisation may be used if needle tip disappears from view.
Local Anaesthetic agent is injected near it avoiding injury to the nerve.
There are two techniques for needle insertion-
- In-plane
- Out-of-plane
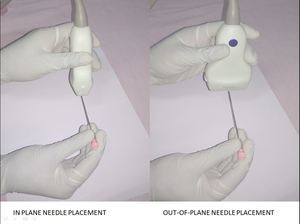
Fig. 3: Techniques of Needle Placement - In-Plane and Out-of-Plane Needle Placement
| Supraclavicular Brachial Plexus Block |
Patient Position: Position the patient supine with back slightly elevated.
The head should be turned away from the side to be blocked and the arm placed at the side.
Needle Size: 22 to 17-gauge,
70 to 100-mm block needle
Volume: 20 to 40-mL local anesthetic
Anatomic Landmarks ::Important surface landmarks include the sternocleidomastoid (SCM) and clavicle.
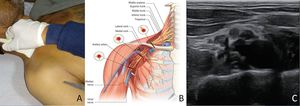
Fig. 4: SupraClavicular Brachial Plexus Block : A-Positioning of transducer in transverse position just above clavicle B- Illustration of relations of Brachial plexus and Subclavian Artery C-Ultrasound Image
References: A,C - Department of Radiodiagnosis & Imaging, AIIMS Bhopal ; B - Anaesthesia Key
Approach & Technique : With a HF linear ultrasound transducer positioned cephalad and medial to the midpoint of the clavicle and oriented vertically,
the brachial plexus is visualized in short-axis posterolateral to the subclavian artery.
After sterile skin preparation,
a local anesthetic skin wheal is raised lateral to the ultrasound transducer.
The block needle is inserted through the skin wheal and directed antero-medially toward the subclavian artery.
To ensure blockade of the C8 and T1 divisions for complete upper extremity anesthesia,
the needle tip should be directed into the “corner pocket” between the posterolateral portion of the subclavian artery and first rib.
The total volume of local anesthetic can be injected incrementally after negative aspiration for blood until the injectate is visualized surrounding the entire plexus
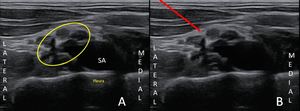
Fig. 5: A- Sonoanatomy Supraclavicular Brachial Plexus:Yellow Circle Brachial Plexus, SA Subclavian Artery , B- Red Arrow:Path of needle
Patient Position: Position the patient supine.
The leg should be straight and not internally or externally rotated.
Needle Size: 22 to 17 gauge,
50 to 100 mm block needle
Volume: 20 to 40 mL local anesthetic
Anatomic Landmarks : The important landmarks for this block include the inguinal crease and femoral artery .
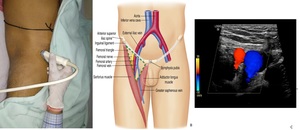
Fig. 6: Femoral Nerve Block : A- Surface landmarks (Probe in Inguinal Crease) , B- Illustration of femoral nerve relations , C- Sonographics Image
References: A,C - Department of Radiodiagnosis & Imaging, AIIMS Bhopal ; B - Elsevier
Approach & Technique : With a high frequency linear transducer positioned at the level of the inguinal crease and oriented parallel to the inguinal ligament,
the FA is identified.
If the femoral and profunda femoris arteries are both visible,
move the transducer more cephalad until the two vessels merge to form the common FA.
At this level,
the FN lies lateral to the FA between the fascia illiaca and iliacus muscle.
The block needle is inserted through the skin wheal using in-plane guidance in a lateral-to-medial direction toward the FN.
Once the needle tip has traversed the fascia iliaca lateral to the FN,
local anesthetic is injected incrementally until visual confirmation of injectate spread surrounding the FN is achieved.

Fig. 7: Sono Anatomy :- Lateral to medial FN- Femoral Nerve , FA- Femoral Artery , FV- Femoral Vein ; Red Arrow - indicates needle path (in plane approach)
Patient Position : The patient is positioned prone,
with the arms resting above the head (to rotate the scapula) and a pillow under the abdomen.
If necessary for patient comfort,
sitting or lateral decubitus positioning can also be used.
Needle size : 22 to 17 gauge,
50 to 100 mm block needle
Volume : 5 to 10 ml of Local anaesthetic
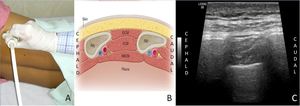
Fig. 8: Intercostal Nerve Block : A- Patient positioning in lateral position B- Illustration of relations of intercostal nerves C- Sonographic image
References: A,C - Department of Radiodiagnosis & Imaging, AIIMS Bhopal ; B - Cousins & Bridenbaugh, 1998
Approach & Technique :Place the ultrasound transducer 3-4 cm from the spinous process in a sagittal plane .
The rib is visualized as a dark shadow; the pleura and lung are visualized below the intercostal space,
deep to the rib.
The rib can be confirmed by sliding the probe toward the midline to visualize the transition of the rib into the transverse process of the spine.
Insert the needle either in plane or out of plane to the transducer and advance to place the tip just below the inferior border of the rib.
After negative aspiration,
inject 3 to 5 mL of LA; as the drug is injected,
the pleura can be seen moving away.
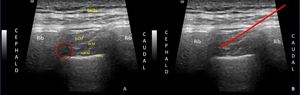
Fig. 9: A- Sono anatomy B- Needle path for intercostal nerve block
| Advantages of Image Guided Regional Analgesia ? |
- Reduced placement time & onset of block
- Reduced quantity of LA required (less toxicity)
- Reduced chances of Vascular puncture
- Useful in high risk patients and patients with challenging anatomy (obese patients)
| Complications of Regional Analgesia ? |
Complications include :-
- Nerve Injury
- Hematoma formation
- LA systemic toxicity - LAST
- Allergic reaction
- Urticaria & Anaphylaxis
- Infection
- Secondary Injury






 , B- Illustration of femoral nerve relations , C- Sonographics Image References: A,C - Department of Radiodiagnosis & Imaging, AIIMS Bhopal ; B - Elsevier")
")

