Jinnah Postgraduate Medical Centre is a tertiary care center where we receive a large number of referrals from the pulmonary clinic for evaluation of respiratory symptoms. We wish to share a series of 33 cases of Hut lung disease,
in Pakistani rural population with a long-term biomass exposure in poorly ventilated environments.
To our knowledge,
this is the first reported series from Pakistan describing the HRCT chest findings in such a large number of patients of Hut lung disease.
In our series,
majority of the patients were females.
All patients had a common history of long-term biomass exposure from indoor combustion of charcoal. None of the patient had history of industrial exposure,
mining exposure or pulmonary tuberculosis. Our patients denied any complain of fever,
chills,
sweats,
weight loss,
eye pain,
arthralgias,
rash,
or sinusitis.
They had no pets at home and no environmental tobacco smoke exposures were reported.
Patients with hut lung can present with a wide spectrum of symptoms,
ranging from quite benign to severe productive cough,
mild dyspnea,
chronic productive cough,
pulmonary hypertension and cor pulmonale.
Other common findings included cyanosis,
crackles,
hepatomegaly,
and edema.5 In our series,
the most common symptoms were of dyspnea and productive cough.
We performed HRCT Chest on Toshiba Asteion 64 slice CT scanner without intravenous contrast using 1 mm collimation every 1 cm from the apex of the lung to the base.
Findings were analyzed on Synapse.
Radiological imaging revealed a wide spectrum of findings.
Some of the common findings included randomly distributed small intrapulmonary nodules which were present in 85% cases,
inter and intralobular septal thinking seen in 73% cases,
ground glass haze seen in 66% cases and fibroatelectatic changes leading to para septal emphysema and fibrotic masses oriented parallel to the fissures giving appearances of progressive massive fibrosis seen in 62% cases.
Almost 85% patients showed hyperdense calcified mediastinal and hilar lymph nodes.
Pleural thickening with non-infective minimal to mild pleural effusions were seen in 15% cases.
All patients underwent bronchoscopy with bronchoalveolar lavage.
Samples were sent for AFB,
C/S,
fungal culture and cytology.
Bronchoscopic results showed inflamed and distorted bronchi with typical dark-black anthracotic plaques invading the large and medium sized airways in virtually all patients (100%).
Bronchoalveolar lavage showed normal cell differential counts.
None of the patients were found to be positive for tuberculous bacillus.
These patients were diagnosed with “hut lung disease”. We would like to share some of our cases:
Case 1: A 57 years old adult female presented with slowly progressing dyspnea and productive cough for 12 years. HRCT revealed fibroatelactatic changes in bilateral apical regions with marked thickening of the oblique fissure and multiple calcified granulomas.
Bronchoscopy showed marked anthracotic plaques.
Patient was diagnosed with Hut lung disease.
[Fig.
1]
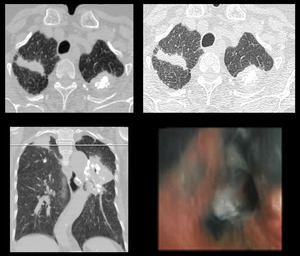
Fig. 1: HRCT: Fibroatelactatic changes in bilateral apical region marked thickening of the oblique fissure on left side and multiple calcified granulomas. Bronchoscopy showed anthracotic ahanges.
Case 2: A 58 years old elderly female presented with slowly progressing dyspnea and productive cough for 12 years. HRCT demonstrated thickened major fissure in the left lung with traction bronchiectasis and a small interstitial nodule.
Bronchoscopy showed marked anthracosis.
Patient was diagnosed with Hut lung disease. [Fig.
2]
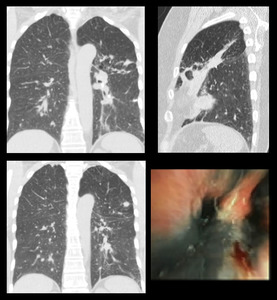
Fig. 2: HRCT: Thickened major fissure in the left lung with traction bronchiectasis and a small interstitial nodule. Bronchoscopy showed marked anthracosis.
Case 3: A 48 years old adult female presented with slowly progressing dyspnea and productive cough for 2 years.
Her HRCT showed enlarged calcified mediastinal lymph nodes with fibrotic changes in bilateral perihilar regions.
Bronchoscopy was performed which showed marked anthracotic changes.
Patient was diagnosed with Hut lung disease. [Fig.
3]

Fig. 3: HRCT: Enlarged calcified mediastinal lymph nodes with fibrotic changes in bilateral perihilar regions. Bronchoscopy show marked anthracotic changes.
Case 4: A 56 years old adult female presented with shortness or breath and productive cough for 10 years. HRCT chest revealed multiple enlarged calcified mediastinal lymph nodes with fibroatelactatic changes in bilateral perihilar regions,
more on left side.
Bronchoscopy show marked anthracotic plaques.
Patient was diagnosed with Hut lung disease. [Fig.
4]
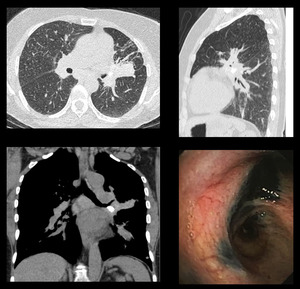
Fig. 4: HRCT: Multiple enlarged calcified mediastinal lymph nodes. Fibrotic changes in bilateral perihilar regions more on left side. Bronchoscopy show marked anthracotic changes.
Case 5: A 62 years old elderly female presented with severe shortness of breath and productive cough for 5 years. HRCT showed fibrotic scar in right lung with calcified mediastinal lymph nodes.
Bronchoscopy showed marked anthracotic changes.
Patient was diagnosed with Hut lung disease. [Fig.
5]
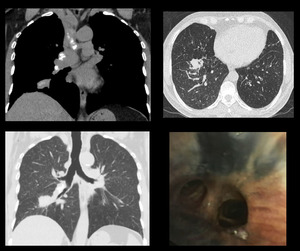
Fig. 5: HRCT: Fibrotic scar in right lung with calcified mediastinal lymph nodes. Bronchoscopy show marked anthracotic changes.
Case 6: A 55 years old adult female presented with chronic productive cough and dyspnea for 2 years.
HRCT revealed basal fibrosis with honey combing,
multiple interstitial lung nodules and subsegmental consolidation.
Brronchoscopy showed anthracotic plaques.
Patient was diagnosed with Hut lung disease. [Fig.
6]
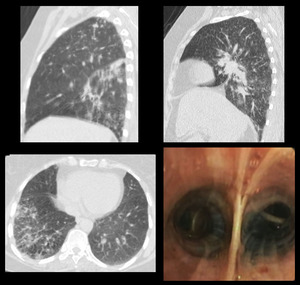
Fig. 6: HRCT: Basal fibrosis with honey combing, interstitial lung nodules and subsegmental consolidation. BRronchoscopy show anthracotic plaques.
Case 7: A 49 years old adult female presented with dyspnea,
chest tightedness and productive cough for 3 years. HRCT revealed fibrotic scar in the right lower lung with calcified mediastinal lymph nodes.
Bronchoscopy showed marked anthracotic changes.
Patient was diagnosed with Hut lung disease. [Fig.
7]
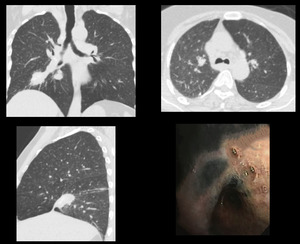
Fig. 7: HRCT: Fibrotic scar in right lower lung along the oblique fissure with ground glass haze. Bronchoscopy show anthrasis.
Case 8: A 70 years old elderly female presented with dyspnea and chronic productive cough for many years. HRCT revealed patchy ground glass haze with basal fibroatelactatic changes and calcified hilar and subcarinal lymph nodes.
Bronchoscopy showed anthracotis changes.
Patient was diagnosed with Hut lung disease. [Fig.
8]
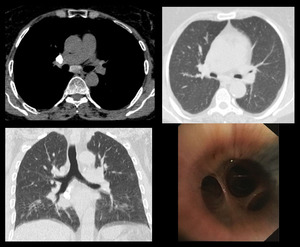
Fig. 8: HRCT: Ground glass haze with basal fibrotic changes and calcified hilar and subcarinal lymph nodes. Bronchoscopy show anthracotis changes.
Case 9: A 61 years old elderly female presented with shortness of breath and chronic productive cough for many years. HRCT showed a patch of consolidation in right lower lobe with perihilar infiltrates and fluffy air space shadowing in the posterior segment of right lower lobe.
Patient was diagnosed with Hut lung disease with superadded pulmonary infection.
Bronchoscopy show anthracotic plaques. [Fig.
9]
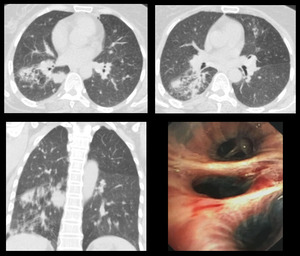
Fig. 9: HRCT: Patch of consolidation in right lower lobe with perihilar infiltrates and fluffy air space shadowing in the posterior segment of right lower lobe. Bronchoscopy show anthracotic plaques.









