We revised in our hospital files all aortic aneurysms that had been operated in our center in the last 5 years.
In total 323 cases were found and only 19 of them had histological proven diagnosis of aortitis: 5 IgG4-Related Disease Aortitis,
5 Takaysus artertitis,
1 Giant Cell arteritis,
2 piogenic aortitis,
4 micotic aneurysms and 2 chronic periaortitis.
Aortitis can be broadly classified as infectious or non-infectious due to practical clinical purposes as this two entities involve different inmmediate therapeutic consequences.
It is important to recall that non-infectious aortitis may be part of a small-,
medium- or large-vessel vasculitis.
NONINFECTIOUS AORTITIS
Noninfectious aortitis is much more common than infectious aortitis,
being the vast majority of cases associated with rheumatic disease.
The most frequent associations are with Takayasu arteritis,
Giant Cell Arteritis,
long-standing ankylosing spondylitis,
Cogan syndrome and Relapsing polychondritis.
There is also a less frequent but well-documented association between aortitis and rheumatoid arthritis,
seronegative spondyloarthropathies,
Behçet's disease,
SLE,
Sarcoidosis,
Wegener's granulomatosis,
polyarteritis nodosa and juvenile rheumatoid.
TAKAYASU ARTERITIS
Takayasu arteritis is a necrotizing and obliterative segmental,
large-vessel panarteritis of unknown cause,
involving elastic arteries including the aorta and its branches.
The first step of the pathological change in TA is granulomatous inflammation of vascular adventitia and outer part of the media.
In particular, severe inflammation of the vasa vasorum is a typical feature of TA.
The inflammatory process begins with perivascular cuffing of the vasa vasorum in the early stage of the disease followed by fibrosis and calcifications in later stages.
It is more common in females of asian origin and the peak incidence is in the 3rd decade of life. Takayasu arteritis is diagnosed based on the 1990 American College of Rheumatology criteria.
Table 3 (Fig.3).

Fig. 3
If three out of six criteria are present,
the sensitivity and specificity for the diagnosis according to these criteria are 90 % and 98 % respectively.
Another laboratory tests such as erythrocyte sedimentation rate and C-reactive protein are elevated more frequently in the acute stage of the disease.
The principal limitation,
however,
is that patients with early nonocclusive disease may not meet the criteria,
and therefore sometimes diagnosis is delayed.
There is no specific clinical biomarker to monitor the disease.
Imaging plays an important role in diagnosis,
management and follow-up.
As it is shown in Table 2 (Fig. 2) multimodality techniques have their utility in diagnosis,
monitoring and even treatment of the disease.
Nowadays however the technique of choice is cross-sectional imaging being CT the most frequently used.
Aortic involvement in TA is common,
with the abdominal aorta affected more often followed by the descending aorta and aortic arch.Fig.4
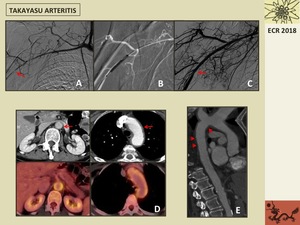
Fig. 4: 60 year-old patient with Takayasu arteritis. A. Angiogram shows a severe long segment stenosis at the right axillary artery (arrow). B. Catheter angiogram shows endovascular treatment performed immediately after the diagnosis with balloon angioplasty. C. Postprocedural angiogram shows a good result with minimal residual stenosis (arrow). D. Postcontrast CT axial images show thickening of aortic wall at the aortic arch and at the abdominal aorta (arrows) and aortic wall FDG uptake at the PET/TC images suggesting inflammatory activity. C. Sagittal reformatted luminal CT image show extensive thickening of thoracic aortic wall (arrows).
The most frequent CT findings are circumferential vessel wall thickening,
thrombosis,
stenosis,
occlusion,
vessel ectasia,
aneurysms and ulcers.
The “double ring” appearance of the thickened aortic wall at contrast-enhanced CT is an early stage finding with a poorly enhanced internal ring of swollen intima and an enhancing outer ring of the inflamed media and adventitia.
MR can demonstrate early wall thickening before luminal narrowing occurs.
PET as mentioned earlier can depict activity and monitor the disease.
Figs.5,6.

Fig. 5: 56-year old patient with Takayasu Arteritis. A,B. Axial T1 FSE weighted images showing thickening of the aortic arch wall (arrows). C. Maximum-intensity-projection coronal MR angiogram showing occlusion of the proximal segment of the left subclavian artery at an early stage of the disease. D-F. CT sagittal postcontrast image and volume rendering reformatted images show occlusion, mild dilatation and calcification of the left subclavian artery at its origin at a late stage of the disease (arrows).

Fig. 6: 27 year-old patient with Takayasu arteritis with extensive affectation of the supra-aortic trunks before and after treatment. A. Coronal maximum-intensity-projection MR angiogram show occlusion of both left carotid and subclavian arteries from their origin with distal recanalization (arrow). B. Coronal postcontrast CT reformatted image show occlusion of both proximal segments of carotid arteries with distal recanalization (circles). C. Coronal maximum-intensity-projection MR angiogram show permeability of left subclavian artery with a stent (circle) and right subclavian artery stenosis (arrow). D. Coronal postcontrast CT reformatted image show stents at both carotid arteries (arrows).
It has been extensively debated if TA and GCA would represent skewed phenotypes within the spectrum of a single disorder.
These two conditions affect both the aorta and its major branches,
are mostly indistinguishable at the histopathologic evaluation and are mainly due to an unregulated inflammatory process.
There are some features such as the age of presentation that can help to differentiate them.
TA treatment is based on medical (corticosteroids and inmmunosuppressive agents) and operative (endovascular or surgical) therapies.
GIANT CELL ARTERITIS
GCA also known as temporal arteritis,
is an elastic vessel systemic granulomatous vasculitis affecting the aorta as well as its secondary and tertiary branches (large and medium-sized vessels) and usually involves extracranial arteries.
Aortic involvement occurs in 15% of GCA patients.
If almost exclusively affects patients above 50 years old,
with women predilection.
Vascular involvement is tipically segmentary,
alternating pathological and spared areas.
It is characterized by disruption of internal elastic lamina with inflammatory cells consisting of multinucleated giant cells and lymphocites.
GCA is diagnosed based on the 1990 American College of Rheumatology criteria where three out of five criteria are required for diagnosis.
Table 4 (Fig.7).

Fig. 7
Long segment involvement with significant wall thickening and smooth tapering proximal and distal to the lesion on CT and MR are classic radiological findings.
The most frequently affected arteries are external cranial branches (especially the superior temporal artery),
the subclavian,
axillary,
femoral,
popliteal,
tibial and peroneal,
with rare involvement of coronary arteries.
In the aorta it can cause luminal changes similar to TA such as stenosis,
occlusion and more frequently dilatation and aneurysm formation. It can also manifest as acute dissection and aortic valve insufficiency. Fig.8

Fig. 8: 76-year-old patient with Giant Cell Arteritis. A. Coronal postcontrast CT reformatted image show a saccular aneurysm at the aortic arch (arrow), elongation and mild dilatation of left subclavian artery (short arrow), and thickening of artic wall. B. Axial postcontrast CT image show a tortuous aortic arch presenting two saccular aneurysms (arrows). C. Axial postcontrast CT at a cranial level of aortic arch showing wall thickening and small luminal projections (arrow). D. Axial PET/TC image showing FDG uptake at the saccular aortic arch aneurysm wall suggesting inflammatory activity (arrow). E. H&E 4x Inflammatory cell infiltrate at the tunica media of the aorta with giant cells (arrows).
Treatment depends on the clinical symptoms and the course of the disease,
being corticosteroids the most frequently used.
Unlike TA,
additional immunosuppressive therapy does not affect the course of the disease.
ANKYLOSING SPONDYLITIS
This HLA-B27 spondyloarthropathy was the first rheumatic disease found to be associated with aortitis.
It usually affects young men and its typical clinical manifestations are back pain and stiffness which worsens with inactivity.
Acute anterior uveitis and also constitutional symptoms are also associated.
Aortic involvement usually affects the aortic root and the aortic valve causing valvular insufficiency,
which is associated with significant morbidity and death.
COGAN SYNDROME
It is an autoimmune disease that causes ocular,
inner ear and vascular inflammation.
It affects young white adults.
Cardiovascular manifestations include aortitis complicated by aortic insufficiency and necrotizing vasculitis,
which may induce coronary,
iliac or renal artery astenosis.
RELAPSING POLYCHONDRITIS
This entity,
characterized by recurrent episodes of connective tissue inflammation and degeneration,
has an immune-mediated origin.
Vascular involvement includes aortic dilatation and regurgitation,
mitra insufficiency and aortitis.
Aortic wall calcification and ossification as well as aneurysm formation have also been described.
UNCOMMON BUT WELL DOCUMENTED AORTITIS ASSOCIATED WITH RHEUMATIC DISEASES
Behcet disease, characterized by the clinical triad of bucal ulcers,
genital ulcers and uveitis.
It is more common in the Mediterranean region (notably in Turkey),
among young males and has a strong association with HLA-B51 serotype. The aorta is the less frequent vascular organ affected (more frequently are venous),
manifesting as aortitis,
aneurysms,
and less frequently thrombosis.
The most life-threating condition in this disease is the rupture of a large aortic or arterial aneurysm.
Aortitis is rare in Rheumatoid arthritis and may be associated with rheumatoid vasculitis in other vessels.
Systemic lupus erythematosus affects the cardiovascular system mostly as serositis of pericardium.
Aortitis is uncommon and it is associated with aortic dissection,
thrombus and aneurysm formation.
OTHER NON-RHEUMATOLOGICAL DISORDERS
ERDHEIM CHESTER SYNDROME
This is a rere form of non-Langherhans cell histiocytosis of unknown origin with relatively uncommon vascular involvement although its frequency is thought to be underestimated as it can be asymptomatic.
CT tipically shows a periaortic tissue,
extending from the ascending aorta to the iliac junction and creating the appearance of a “coated aorta”.
It can also extend to supraaortic trunks and abdominal branches.
PARANEOPLASTIC AORTITIS
Autoinmune manifestations in myelodysplastic syndromes have been described.
If present usually associate a por prognosis.
These manifestations include usually small vessel vasculitis.
Most cases described in the literature were stablished simultanously with patients with a myelodisplastic syndrome.
In all cases described patients had remarkable systemic inflammatory symptoms.
At imaging the reported cases showed diffuse thickening of the aortic wall including or not its branches.
CARCINOID SYNDROME
Some malignancies have also been described as potential causes of secondary periaortitis (previously referred as retroperitoneal fibrosis).
Most of the times,
it is the consequence of a prominent desmoplastic response of retroperitoneal metastases (e.g.,
prostate,
breast,
colon carcinoma) or of a primary retroperitoneal tumor (e.g.,
Hodgkin's and non-Hodgkin lymphomas among others).
The only exception are carcinoids,
that are likely to induce periaortic fibrosis in the absence of metastases,
probably through a mechanism mediated by serotonin or by the release of profibrogenic growth factors.
Fig.9

Fig. 9: 67 year-old patient with a neuroendocrine tumor. A. Axial CT with intravenous and oral contrast showing a small ileal tumor conditioning small bowel dilatation (arrow). B. Axial postcontrast CT showing thickening of the ascending aortic wall (arrow). C-E. Coronal and axial CT images show prominent thickening of abdominal aortic wall (arrows) and important FDG uptake at PET/TC image.
Another well-known potential manifestation in carcinoid disease due to this mechanism (usually in carcinoid tumors with liver metastatic disease) is cardiac involvement (Hedinger syndrome) that results in right-sided valvular fibrosis leading to tricuspid insufficiency and pulmonary stenosis.
IgG4-RELATED DISEASE
Immunoglobulin 4-Related Disease is a chronic systemic inflammatory disease that affect various systems,
including the cardiovascular (CV) system.
Assessment of serum IgG4 levels and involved organ biopsy are necessary for diagnosis.
IgG4-Related Disease is characterized by fibrosclerosis,
lymphocytic infiltration and presence of IgG4-positive plasma cells.
IgG4-RD involves different organs such as the pancreas (the first organ in which this disease was described as autoinmune pancreatitis-AIP),
kidneys,
biliary tree,
lacrimal glands (Mickulicz´s disease),
retroperitoneum (retroperitoneal fibrosis also called Ormond´s disease),
aorta (aortic aneurysm and aortitis) and heart (constrictive pericarditis,
and pseudotumors around the coronary arteries).
Fig.10.

Fig. 11: 30 year-old patient with IgG4-Related Aortitis. A. Simple chest x-ray showing a prominent thoracic aorta with a tortuous shape and small apical nodular opacities that proved to be tuberculosis. B. Axial postcontrast CT image show a tortuous and aneurysmatic ascending and descending thoracic aorta with mild thickening of the aortic wall. C. Axial CT-image show intimo-medial flaps at the descending thoracic aorta (arrow). D-G. Sagittal reformatted CT images and volume rendering reformatted images showing the extension of the disease, affecting from the aortic root to almost the distal descending thoracic aorta.
Clinical presentation differs depending on the organ affected but usually is poorly expressive with mild localized symptoms and organ failure.
Inflammatory periarteritis (chronic periaortitis) usually presents with back or abdominal pain and elevation of blood inflammatory indices (PCR,
ESR).
Retroperitoneal fibrosis can be secondary to drugs,
infections,
radiation,
surgery and malignacies,
but 2/3 of cases the etiology is unknown.
It is characterized by a fibro-inflammatory soft tissue mass surrounding the aorta and/or adjacent tissues. Fig.11.

Fig. 12: 69 year-old patient with IgG4-Related Aortitis. A. Axial precontrast CT image showing prominent thickening of the aortic wall with no significant density (arrow). B. Axial postcontrast CT showing important thickening of the ascending aortic wall (arrow). C. Coronal postcontrast reformatted image show the thickening along the ascending aortic wall and supraaortic trunks (arrow). D. Sagittal postcontrast reformatted image after surgery showing supracoronary ascending aorta replacement and a prosthetic aortic valve. E. Inmunostaining demonstrating plasma cells expressing IgG4+ (small brown cells).
IgG4-sclerosing lymphoplasmacytic histology is aconsistent finding of thoracic Inflammatory Aortic Aneurysms (IAAs).
IgG4-RD can lead to Aneurysm formation in Abdominal Aorta(AAA),
Thoracic Aorta (TAA),
Coronary Arteries (CAA) and/or any other artery.
It is remarkable that sometimes these organs can be affected with normal serum IgG4 and with no other organ involvement at the same time behaving as a localized autoinmune process.
That is why histologic criteria are necessary.
Table 5 (Fig.12)

Fig. 10
The disease usually responds to treatment with corticosteroids and/or immunosuppressive medication.
RADIATION-INDUCED AORTITIS
It can appear more than 10 years after high dose radiation of the aorta and aortic branches.
Changes are normally confined to the radiation field and consist of thrombosis,
pseudoanerysm,
rupture,
stenosis and accelerated wall calcification.
Drug-induced aortitis has also been described with therapeutic agents such as gemcitabine,
minociclyne,
retinoids and leukotriene receptor antagonists.
INFECTIOUS AORTITIS
It is an inflammatory and infectious process affecting the aortic wall and sometimes other vessels.
It is an infrequent process as aortic wall is very resistant to infection,
and it is more frequently affected when it is previously damaged (preexisting aneurysm,
atherosclerotic disease,
cystic medial necrosis,
clinical devices,
radiation,
etc.).
The most frequent pathogens are S.
aureus and Salomonella species.
Other pathogens involved include T.
pallidum,
M tuberculosis,
and other bacteria.
Usually it is the consequence of hematogenous spread,
contiguous seeding from adyacent infection and traumatic or iatrogenic inoculation.
Radiologic manifestations of infectious aortitis include aortic wall thickening,
periaortic fluid or soft-tissue collections,
rapidly progressing saccular aneurysm or pseudoaneurysm,
and occasionally air in the aortic wall.
INFECTED (MYCOTIC) AORTIC ANEURYSM
Mycotic aneurysm is a confusing term referring to all aneurysms with an infectious origin.
Infected aortic aneurysm is a consequence of an infectious aortitis affecting a vulnerable vessel and the most frequent pathogen found is Salmonella. The infectious and inflammatory process weakens the aortic wall leading to disruption creating a false lumen or pseudoaneurysm,
in most 90% cases adopting a saccular morphology.
The most frequent location is the infrarrenal aorta followed by the descending thoracic aorta.
Fig.
13.
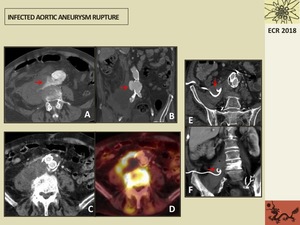
Fig. 13: 88 year-old patient with an acute aortic rupture secondary to an abdominal aortic aneurysm infected with Salmonella. A,B. Axial and coronal postcontrast CT image show rupture of the abdominal aneurysm (arrows) and a large retroperitoneal collection with a heterogeneous density. C. Axial CT image show aortobi-iliac endoprothesis replacement persisting the large retroperitoneal collection at the right periaortic space and bone sclerosis suggesting spondylodiscitis. D. PET/TC axial image showing prominent FDG uptake of the infected collection and bone. E,F. Axial and coronal reformatted postcontrast CT images showing decreasing of the collection that was drained with a Pigtail Catheter (arrows).
Mycotic aneurysms of the aortic root are commonly associated to endocarditis and surgery procedures. Fig.
14
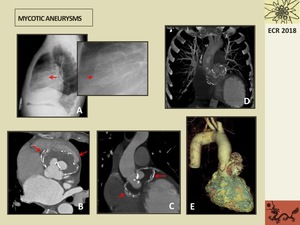
Fig. 14: 49 year-old patient with mycotic aneurysms with history of infectious endocarditis. A. Lateral simple chest x-ray showing linear curved calcifications at the aortic root (arrow). The patient had also an epicardial pacemaker. B,C. Coronal and axial reformatted images show mycotic aneurysms at the aortic root with mural thrombus and wall calcification (arrows). D,E. Coronal volume rendering reformatted images showing the mycotic root aortic aneurysms.
Imaging findings depend on the course of the disease,
in the early fase a periaortic soft-tissue mass or fat stranding can be found before the development of the aneurysm.
If left untreated this disease may have a fatal outcome as it can lead to sepsis,
severe hemorraghe and rupture of the aneurysm.


. B. Catheter angiogram shows endovascular treatment performed immediately after the diagnosis with balloon angioplasty. C. Postprocedural angiogram shows a good result with minimal residual stenosis (arrow). D. Postcontrast CT axial images show thickening of aortic wall at the aortic arch and at the abdominal aorta (arrows) and aortic wall FDG uptake at the PET/TC images suggesting inflammatory activity. C. Sagittal reformatted luminal CT image show extensive thickening of thoracic aortic wall (arrows).")
. C. Maximum-intensity-projection coronal MR angiogram showing occlusion of the proximal segment of the left subclavian artery at an early stage of the disease. D-F. CT sagittal postcontrast image and volume rendering reformatted images show occlusion, mild dilatation and calcification of the left subclavian artery at its origin at a late stage of the disease (arrows).")
. B. Coronal postcontrast CT reformatted image show occlusion of both proximal segments of carotid arteries with distal recanalization (circles). C. Coronal maximum-intensity-projection MR angiogram show permeability of left subclavian artery with a stent (circle) and right subclavian artery stenosis (arrow). D. Coronal postcontrast CT reformatted image show stents at both carotid arteries (arrows).")

, elongation and mild dilatation of left subclavian artery (short arrow), and thickening of artic wall. B. Axial postcontrast CT image show a tortuous aortic arch presenting two saccular aneurysms (arrows). C. Axial postcontrast CT at a cranial level of aortic arch showing wall thickening and small luminal projections (arrow). D. Axial PET/TC image showing FDG uptake at the saccular aortic arch aneurysm wall suggesting inflammatory activity (arrow). E. H&E 4x Inflammatory cell infiltrate at the tunica media of the aorta with giant cells (arrows).")
. B. Axial postcontrast CT showing thickening of the ascending aortic wall (arrow). C-E. Coronal and axial CT images show prominent thickening of abdominal aortic wall (arrows) and important FDG uptake at PET/TC image.")

. D-G. Sagittal reformatted CT images and volume rendering reformatted images showing the extension of the disease, affecting from the aortic root to almost the distal descending thoracic aorta.")
. B. Axial postcontrast CT showing important thickening of the ascending aortic wall (arrow). C. Coronal postcontrast reformatted image show the thickening along the ascending aortic wall and supraaortic trunks (arrow). D. Sagittal postcontrast reformatted image after surgery showing supracoronary ascending aorta replacement and a prosthetic aortic valve. E. Inmunostaining demonstrating plasma cells expressing IgG4+ (small brown cells).")
 and a large retroperitoneal collection with a heterogeneous density. C. Axial CT image show aortobi-iliac endoprothesis replacement persisting the large retroperitoneal collection at the right periaortic space and bone sclerosis suggesting spondylodiscitis. D. PET/TC axial image showing prominent FDG uptake of the infected collection and bone. E,F. Axial and coronal reformatted postcontrast CT images showing decreasing of the collection that was drained with a Pigtail Catheter (arrows).")
. The patient had also an epicardial pacemaker. B,C. Coronal and axial reformatted images show mycotic aneurysms at the aortic root with mural thrombus and wall calcification (arrows). D,E. Coronal volume rendering reformatted images showing the mycotic root aortic aneurysms.")
