Considerations in reviewing CT imaging following penetrating trauma include:
- Identifying the main site of injury and depth of the wound
- Identifying solid organ injury
- Recognising vascular injury
- Review areas
Identifying the main site of injury and depth of the wound
Use of 3D reconstructions and multiplanar reformats is essential to improve diagnostic yield (Figure 1 and 2).
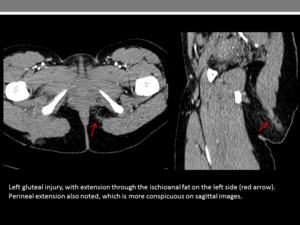
Fig. 1
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
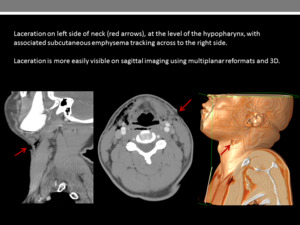
Fig. 2
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Evaluating subcutaneous and intramuscular emphysema can be further clarified using lung and soft tissue windows (Figure 3).
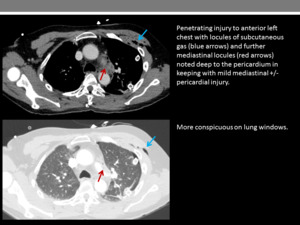
Fig. 3
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Location of haematoma and free fluid can assist in identifying the trajectory and extent of injury (Figure 4).
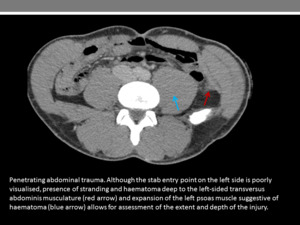
Fig. 4
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Identifying solid organ injury
Multiplanar reformats ensures in-plane tissue disruption is not missed.
Irregular,
linear or branching low attenuation could be consistent with laceration (Figure 5).

Fig. 5
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Poorly defined foci of heterogenous intraparenchymal or subcapsular mixed density fluid suggest haematoma (Figure 6).
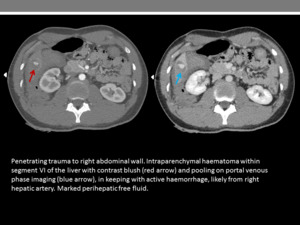
Fig. 6
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Wedge shaped low attenuation can indicate infarction.
Contrast extravasation is consistent with active bleeding within an organ (Figures 6 - 9),
whilst contained vascular injuries may include pseudoaneurysms (Figure 10) and arteriovenous fistulae.
Fig. 6
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
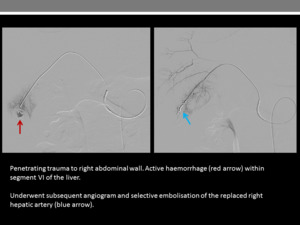
Fig. 7
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
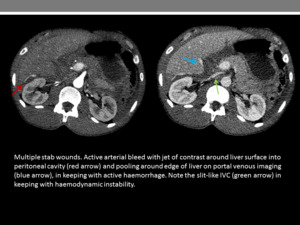
Fig. 8
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
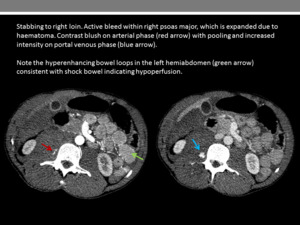
Fig. 9
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
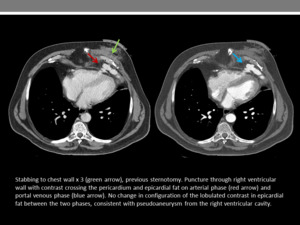
Fig. 10
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Recognising vascular injury
CT allows for assessment of contrast extravasation,
indicating active bleeding,
and abrupt interruption or attenuation of vascular enhancement.
Vascular injuries include laceration,
pseudoaneurysm and arteriovenous fistulae [2] and can be associated with significant haematoma.
Types of vascular injury are demonstrated:
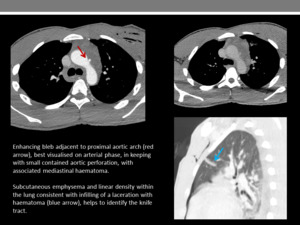
Fig. 11
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
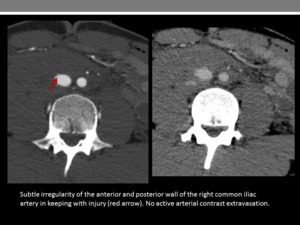
Fig. 12
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
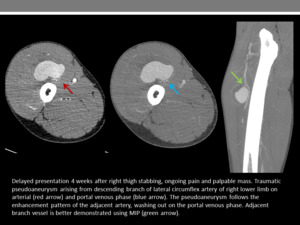
Fig. 13
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK

Fig. 14
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
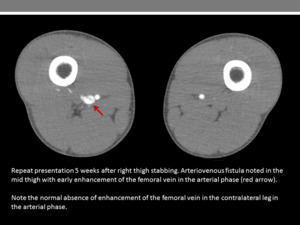
Fig. 15
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
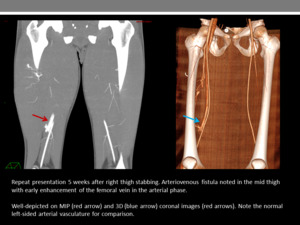
Fig. 16
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
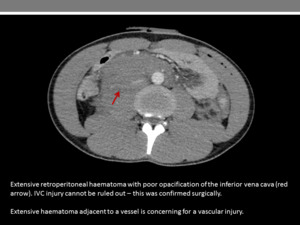
Fig. 17
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Dual phase imaging (arterial and portal venous phase) is the first-line protocol in assessing potential vascular injury and/or active bleeding in the setting of penetrating trauma (Figures 18 and 19) and can detect bleeding rates as low as 0.3ml/min. Other available modalities are catheter angiography,
with detection rates of >0.5ml/min [3],
and RBC scintigraphy. The latter is the most sensitive and is able to detect bleeding rates as low as 0.04ml/s.
However,
limited resolution makes it more difficult to accurately localise bleeding and in the acute setting,
radionuclide imaging is often impractical.
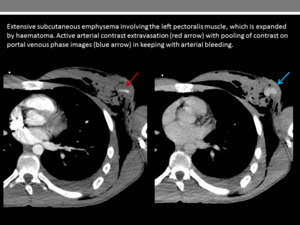
Fig. 18
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
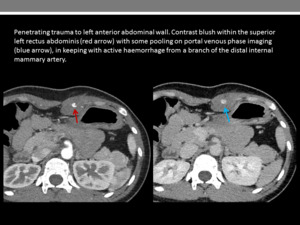
Fig. 19
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Role of interventional radiology [4,
5]:
-
It is imperative for the reporting radiologist to highlight when bleeding is amenable to interventional management.
-
In patients with localised or continued visceral bleeding recognised on CT imaging,
selective endovascular treatment can be considered.
-
Contained vascular injuries such as pseudoaneurysm or arteriovenous fistulae can also be managed using an endovascular approach,
as well as points of focal active vascular bleeding.
-
Superficial bleeding may be amenable to direct compression or minimally invasive surgical exploration.
-
Transection requires a direct surgical approach.
-
Intimal or contained vascular injuries injuries do not usually require intervention.
Review areas
CT can be insensitive at detecting bowel and diaphragmatic injuries.
Diaphragmatic injuries
CT features of diaphragmatic injury include:
-
Collar sign: Narrowed appearance of herniated contents at the point of the diaphragmatic defect,
forming an ‘hourglass’ configuration.
-
Dependent viscera sign: Lack of interposition of lung or pleura between herniated contents and chest wall means herniated contents usually lie posteriorly when lying supine.
-
Interruption or thickening of diaphragm (Figure 20).
-
Contiguous injuries either side of the diaphragm indicate trauma.
On the right side in particular,
herniation is less common as the liver abuts the defect,
so adjacent injuries may be the only radiological feature (Figures 21 and 22).
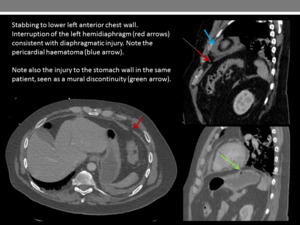
Fig. 20
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
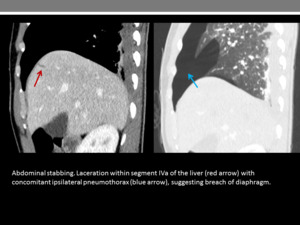
Fig. 21
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
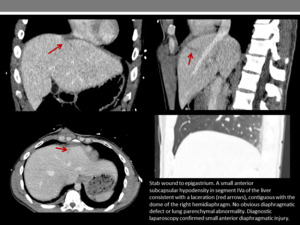
Fig. 22
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Bowel injuries
CT features of bowel injury include:
-
Peritoneal breach (Figure 23)
-
Free intraperitoneal fluid - peritoneal or retroperitoneal haematoma would indicate peritoneal breach even if the breach itself is not visible,
and this should warrant diagnostic laparoscopy (Figure 24)
-
Free intraperitoneal air (Figure 25) - however,
it is important to note intraperitoneal air can be introduced via the wound tract
-
Bowel wall thickening or abnormal enhancement (Figure 26)
-
Bowel wall defect (Figure 27)
-
Wound tract extending to bowel
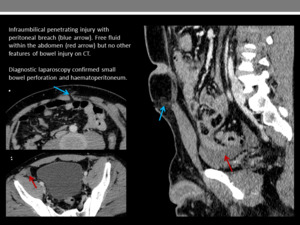
Fig. 23
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
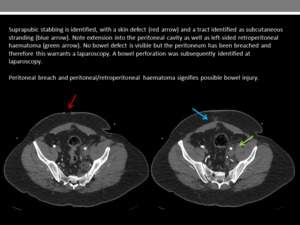
Fig. 24
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
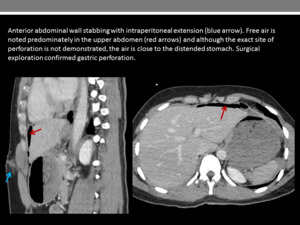
Fig. 25
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
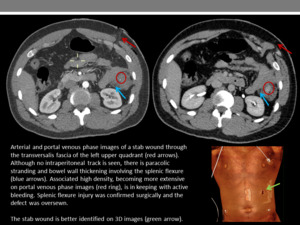
Fig. 26
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Fig. 27
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Other considerations
Particularly in relation to penetrating injuries,
which are not always immediately visible on imaging,
we would advocate in-depth discussion with the clinical teams to obtain an understanding about the location and mechanism of injury.
In our Trust,
the on-call radiologist is present at the time of scanning of trauma patients,
to facilitate discussion with the trauma team.
