Definition:
Thoracic outlet syndrome (TOS) is a group of clinical syndromes caused by position-dependent compression of the subclavian vessels (vascular TOS) or the brachial plexus (neurogenic TOS),
most commonly in the costoclavicular space.
Neurogenic TOS is much more common than vascular TOS,
and venous TOS,
which is due to subclavian vein compression,
is more common than arterial TOS,
which is due to subclavian artery compression.
TOS is most common in younger women.
Compression Locations:
The three most common sites of neurovascular compression in TOS are:
- Interscalene triangle: defined by the first rib and the anterior and middle scalene muscles.
It is the most medial site of neurovascular compression in TOS.
The subclavian artery and branches of the brachial plexus pass through the interscalene triangle,
whereas the subclavian vein passes anterior to it.
- Costoclavicular space: between the clavicle and first rib.
- Subpectoral space (also called the retropectoralis minor space or subcoracoid tunnel): between the pectoralis minor muscle and coracoid process.
Etiology of thoracic outlet syndrome
Common causes of TOS include:
- Scalenus anticus syndrome: abnormal insertion of scalenus anterior onto first rib (most common cause)
- Congenital cervical rib
- Bony abnormality of first rib or clavicle (congenital anomaly,
malunited fracture,
callus,
Paget disease,
tumor)
- Elongated C7 transverse process
- Muscle hypertrophy
- Fibrous bands
- Supraclavicular tumor or lymphadenopathy
Establishing the diagnosis
The diagnosis of TOS is made by history and physical exam.
Imaging studies can only support the diagnosis and suggest an etiology. Provocative tests are usually needed,
such as imaging with the arm in multiple positions.
However,
positional changes in vessel caliber without corresponding symptoms are not diagnostic of TOS.
Studies such as electrodiagnostic tests and brachial plexus neurography can also be helpful.
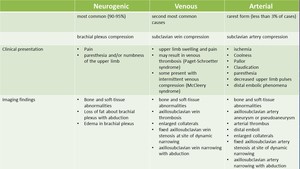
Fig. 1: Thoracic outlet syndrome (TOS) is caused by compression of either the subclavian vessels (vascular TOS) or the brachial plexus (neurogenic TOS). This table highlights the difference between them.
Clinical presentation of venous TOS
Patients with venous TOS may present with upper extremity swelling,
congestion,
edema,
rapid onset skin discoloration,
and pain (see table below).
Venous TOS can progress to spontaneous axillosubclavian thrombosis,
also known as effort thrombosis or Paget-Schroetter syndrome.
The latter can lead to pulmonary embolism or venous gangrene.
Engorged collateral vessels may form across the shoulder and lateral pectoral areas.
Paresthesias and weakness have also been reported.
Clinical presentation of arterial TOS
Early diagnosis and treatment of vascular TOS is important.Arterial TOS may present with symptoms of distal upper extremity ischemia,
such as exertional or positional weakness and fatigue,
limb coldness,
pain and numbness (see table below).
Serious complications of arterial TOS include critical digital ischemia and rarely stroke from retrograde embolism.
Imaging
The role of imaging in TOS is to:
- Identify the neurovascular structure(s) being compressed
- Localize the site of compression
- Identify the anatomic cause of compression
- Exclude TOS mimics
Imaging with ultrasound,
contrast-enhanced CT,
MRI or conventional angiography is useful for detecting vascular thoracic outlet syndrome in symptomatic patients.
Imaging is typically performed twice: once with one or both arms in the raised (abducted) stress position and then again with the arm(s) at rest in the neutral (adducted) positions for baseline comparison.
Chest Radiography (CXR)
CXR is usually the initial imaging modality in suspected TOS due to widespread availability and low cost.
The primary purpose of the CXR is to evaluate for osseous abnormalities,
such as first rib anomalies,
cervical ribs,
or elongated C7 transverse process.
Arterial TOS is almost always associated with osseous abnormalities of the thoracic outlet.
Soft tissue lesions such as lung cancer may be seen as well.
Digital Subtraction Angiography (DSA)
Historically,
DSA has been considered the gold standard for evaluation of the subclavian vessels.
The two main DSA techniques for TOS are direct arteriography and direct venography of the axillo-subclavian artery and vein,
respectively.
The main limitation of DSA is an inability to identify the impinging structures.
DSA is now used mostly to guide interventions.
Magnetic resonance imaging (MRI) and MR Angiography (MRA)
Unlike DSA,
MRI and MRA are noninvasive and do not expose the patient to ionizing radiation,
yet still provide robust,
reliable and reproducible diagnostic information.
MRI and MRA can accurately evaluate upper limb arterial and venous thrombosis.
T1- and T2-weighted MRI sequences in the sagittal and axial planes help to delineate musculoskeletal anatomy and identify potential sites of neurovascular impingement.
The MR studies are performed with one or both arms in the neutral and abducted positions.
There are at least four MRA techniques that can be used to evaluate vascular TOS:
- 3D MR angiography (MRA)
- Direct 3D MR venography (MRV)
- Time-resolved 3D MR Angiography (TR-MRA)
- 2D time-of-flight MRA.
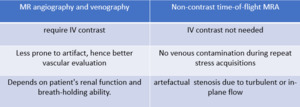
Fig. 2: Table highlighting the differences between contrast enhanced MRA/MRV and non contrast time of flight MRA.
Time-Resolved 3D MR Angiography (TR-MRA)
Recently Time-Resolved 3D MR Angiography (TR-MRA) has been shown to be an excellent noninvasive alternative to DSA in patients with suspected vascular TOS.
It obviates the need for contrast bolus timing,
which is required for single phase contrast-enhanced 3D MRA and MRV.
By comparison,
TR-MRA enables quasi-real time imaging of the intravascular contrast bolus with only a small contrast dose.
The technique reliably captures arterial phase,
mixed phase and venous phase images with reasonably high temporal and spatial resolution.
It can evaluate flow dynamics in arteries,
veins or both.

Fig. 3: Coronal MIP cine loop from contrast-enhanced time-resolved 3D MRA shows focal stenosis of the right subclavian artery with the right arm raised overhead (A).

Fig. 4: The stenosis resolves with the right arm down (B)
TR-MRA is especially useful when:
- The contrast bolus arrival time in a specific arterial or venous bed is uncertain
- The patient is freely breathing
- The contrast flow dynamics are critical to establishing a diagnosis.
TR-MRA can provide useful anatomic and functional information about complicated vascular lesions and identify postoperative complications,
such as residual vascular stenosis or restenosis.
In patients with suspected vascular TOS,
provocative arm positions can be employed to reveal the presence and degree of vascular impingement.
Separate image acquisitions are performed with one or both arms adducted (neutral position) and abducted with external rotation (stress position) to elicit positional vascular narrowing and precisely locate the site of vascular compression.
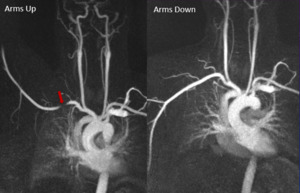
Fig. 5: Coronal MIP images from a 3D TR-MRA show stenoses of the right subclavian artery with the right arm up (left panel, red arrows). The stenosis resolves with the right arm down (right panel). Findings are consistent with right-side arterial TOS.
To perform TR-MRA on a patient with suspected unilateral arterial TOS,
the contralateral arm is injected with undiluted gadolinium-based contrast agent (GBCA).
The reason for injecting the contralateral arm is to avoid the “crossing artifact” in the subclavian artery ipsilateral to the IV injection site.
There are two options for performing TR-MRA on a patient with suspected unilateral or bilateral venous TOS.
- The first option is to use the aforementioned arterial TOS technique,
but allow image acquisition to continue through the venous phase.
- The second (and more elegant) option is to inject the ipsilateral arm (or both arms simultaneously for a bilateral exam) with GBCA diluted 1:10 in saline.
This technique is known as direct MR venography.
The GBCA must be diluted in order to avoid signal loss in the ipsilateral axillary and subclavian veins due to intravascular T2* shortening.
MR Imaging Features of Venous TOS include:
- Axillosubclavian vein thrombosis
- Focal fixed subclavian vein stenosis at a site of dynamic compression
- Expanded collateral vessels
- Positional vascular narrowing
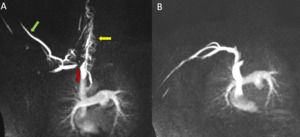
Fig. 6: Coronal MIP images from a direct venous contrast-enhanced TR-MRA show a stenosis of the right subclavian vein with the right arm raised overhead (A). The stenosis resolves when the right arm arm is down (Bl). Findings are consistent with venous TOS. Technologist forgot to put tourniquet on the right arm leading to contrast reflux and opacification of the cephalic vein (green arrow) secondary to the TOS obstruction. Small venous collaterals present in the neck (yellow arrow) suggestive of long standing chronic obstructive process.
MR Imaging Features of Arterial TOS include:
- Axillosubclavian arterial aneurysm or pseudoaneurysm
- Arterial thrombosis
- Focal fixed subclavian artery stenosis at a site of dynamic compression
- Distal emboli
- Enlarged collaterals
- Positional vascular narrowing
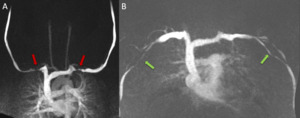
Fig. 7: This is a case of bilateral venous TOS. Coronal MIP images from TR-MRA using bilateral “direct” MR venography technique. There are stenoses of both subclavian veins with the both arms up (A, red arrows). The stenoses resolve with the arms down (Bl). Images were acquired by simultaneously injecting both arms with IV Gadavist diluted 1:10 with saline. Tourniquet applied on both arms (green arrows)

 is caused by compression of either the subclavian vessels (vascular TOS) or the brachial plexus (neurogenic TOS). This table highlights the difference between them.")

.")
")
. The stenosis resolves with the right arm down (right panel). Findings are consistent with right-side arterial TOS.")
. The stenosis resolves when the right arm arm is down (Bl). Findings are consistent with venous TOS. Technologist forgot to put tourniquet on the right arm leading to contrast reflux and opacification of the cephalic vein (green arrow) secondary to the TOS obstruction. Small venous collaterals present in the neck (yellow arrow) suggestive of long standing chronic obstructive process.")
. The stenoses resolve with the arms down (Bl). Images were acquired by simultaneously injecting both arms with IV Gadavist diluted 1:10 with saline. Tourniquet applied on both arms (green arrows)")