GI lymphoma has a wide variety of imaging appearances and definitive diagnosis relies on histopathologic analysis.
However,
certain findings can strongly suggest the diagnosis.
The most commonly used imaging is computed tomography.
1/ Gastric lymphoma:
The stomach is the most frequent site of GI lymphoma accounting for about 50% of cases.
MALT lymphoma is closely associated with chronic inflammation,
such as HP infection and can transform into intermediate or high-grade large cell lymphoma if not diagnosed or treated in time.
CT patterns include:
♦ The infiltrative form:
- It appears as a focal Fig. 1 or diffuse Fig. 2 wall thickening of 2–5 cm with low contrast enhancement and extensive lateral extension of the tumor due to submucosal spread and is associated with lymphadenopathy.
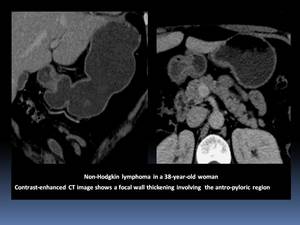
Fig. 1
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.

Fig. 2
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
- Complications such as obstruction,
perforation,
or fistulization Fig. 3 can occur as a result of the disease itself or of the treatment.
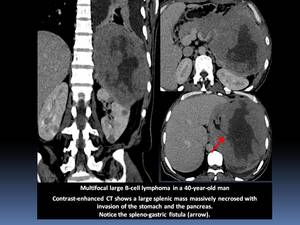
Fig. 3
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
♦ The nodular and ulcerative forms
- The nodular form is characterized by the development of multiple discrete submucosal nodules or masses in the stomach.
- The masses may enlarge and evolve towards ulcerated masses,
known as bull’s-eye or target lesions.
- Extensive necrosis and excavation may be seen,
appearing as giant cavitated lesions. Fig. 4
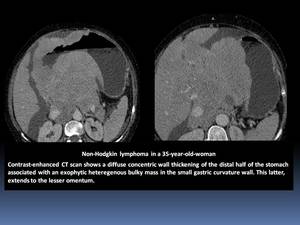
Fig. 4
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
♦ Differential diagnosis:
- Adenocarcinoma is the main differential diagnosis with wall thickenening associated with lymphadenopathy.
- Metastases and Kaposi’s sarcoma are the differential diagnosis for bull’s-eye lesions.
- In favor of the lymphoma diagnosis:
- Preservation of the perigastric fat planes.
- The stomach lumen is preserved,
making gastric obstruction a rather uncommon feature.
- Transpyloric spread is more common in gastric lymphoma,
but it should not be considered to suggest the diagnosis because of the higher incidence of carcinoma.
- The extension of lymphadenopathy below the renal hila and their appearance as bulky masses.
2/ Small-bowel lymphoma:
Lymphoma is the most common malignancy of the small bowel making up to 20% of all tumors in this location.
The distal ileum is the most common site,
owing to the largest amount of lymphoid tissue.
In contrast,
lymphoma complicating celiac disease usually involves the proximal jejunum.
CT allows the evaluation of wall thickness,
mesenteric vasculature,
and any associated extramural finding.
CT-enterography is preferred and is performed after oral administration of an isotonic solution,
in order to obtain an adequate distension of the intestine.
In general,
small-bowel lymphoma manifests as solitary lesion,
but multiple sites are involved in 25% of cases.
Imaging features are variable:
♦ The infiltrative form:
- The most common form,
characterized by segmental symmetrical or slightly asymmetrical infiltrating lesions with a medium thickness of 2 cm.
Fig. 5
- Usually,
the infiltrative lesions show ill-defined margins and a homogeneous contrast enhancement.
- The enhancement may rarely be heterogeneous due to the development of necrosis and/or ischemia.
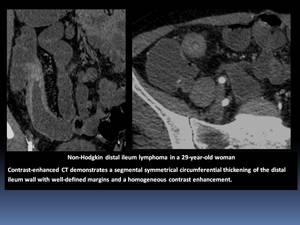
Fig. 5
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
- T-cell lymphoma has a higher prevalence of multifocal involvement and bowel perforation.
Wall thickness is usually moderate,
as opposed to the marked thickening seen in B-cell lymphomas. Fig. 6
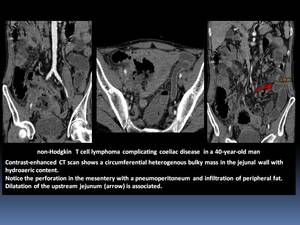
Fig. 6
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
· The aneurismal pattern (diameter of the lumen dilation over 4 cm),
represents 30% of small bowel lymphoma and usually coexists with the infiltrative form since it can represent its natural evolution.
The polypoid form:
- It is characterized by a focal,
polypoid,
homogeneous parietal mass without wall thickening or lymphadenopathy. Fig. 7
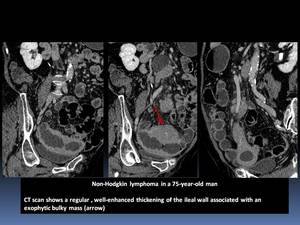
Fig. 7
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
- It can also appear as an intraluminal polypoid Fig. 8 or a large exocentric mass Fig. 9, often associated with extension into the mesentery and regional lymph nodes.
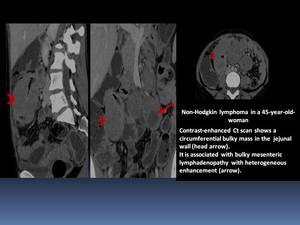
Fig. 8
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
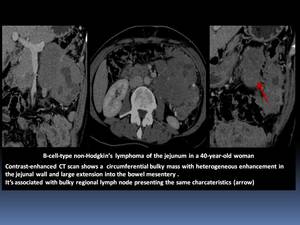
Fig. 9
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
- The tumor may involve a long segment of bowel and may ulcerate and perforate into the adjacent mesentery,
resulting in the formation of a confined,
usually sterile abscess. Fig. 10
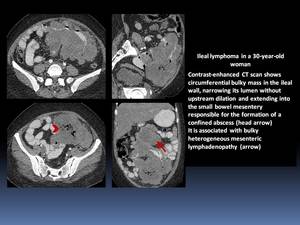
Fig. 10
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
- Bulky mesenteric or retroperitoneal lymphadenopathy and splenomegaly may be seen.
The stenosing form:
- It generally occurs in Hodgkin's lymphoma.
- Stenosis observed in lymphoma are responsible for minimal or no dilation of the upstream bowel segments compared to other malignancies,
due to the absence of a desmoplastic reaction.
Differential diagnosis includes inflammatory (Crohn's disease and intestinal tuberculosis),
neoplastic,
and metastatic lesions.
- Adenocarcinoma : wall thickenening associated with lymphadenopathy.
Fig. 11
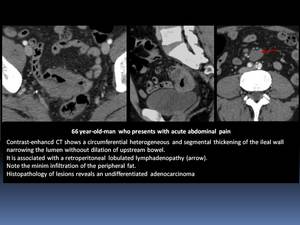
Fig. 11
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
- In front of large necrotic cavitation,
primary carcinoma,
metastases (melanoma and renal cancer),
and the intestinal leiomyosarcoma are the differential diagnosis.
- In favor of the lymphoma diagnosis:
- Significant thickening of the bowel wall (greater than 2 cm).
- Coexistence of perivisceral multiple lymph nodes.
- The aneurysmal form of lymphoma can usually be differentiated from adenocarcinoma by the length of the narrowed segment,
the degree of narrowing and the absence of significant obstruction.
3/ Large bowel:
Colorectal lymphomas represent 6-12% of GI lymphomas.
The cecum is the most frequent site of involvement.
In children,
Burkitt lymphoma is most common,
whereas in adults,
large cell lymphomas and low-grade B-cell lymphomas predominate.
CT patterns include:
The polypoid form:
- The most common pattern,
usually located near the ileocecal valve and tends to spread by direct extension into the terminal ileum.
- Polyps may vary from few millimetres to 20 centimetres and are mainly located in the ileocecal valve.
- Large tumors can excavate into the mesentery Fig. 12
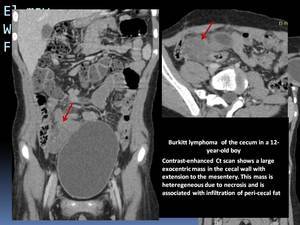
Fig. 12
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
The infiltrative form:
Is characterized by a long segment of concentric narrowing with smooth overlying mucosa and thickened,
irregular haustral folds caused by submucosal tumor infiltration. Fig. 13
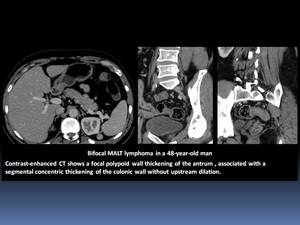
Fig. 13
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
Less frequently:
- Colorectal lymphomas may also present as a focal strictures,
aneurismal dilation,
or ulcerative forms with fistula formation.
- Rectal lymphoma is a rare type of GI lymphoma and is indistinguishable from rectal carcinoma Fig. 14
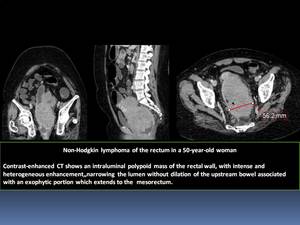
Fig. 14
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
- Lymphoma of the appendix is very rare Fig. 15 Fig. 16
- It is more common to see cecal lymphoma extending to the base of the appendix which becomes massively enlarged with mural thickening.
- It typically maintains its vermiform appearance.
- Aneurysmal dilation of the lumen is sometimes seen.
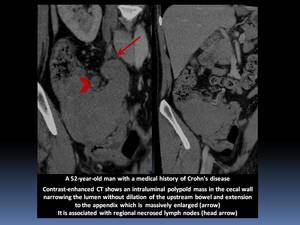
Fig. 15
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
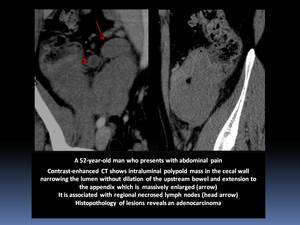
Fig. 16
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
Complications:
- Obstruction is less frequent in lymphoma than in adenocarcinoma.
- Intussusception may occur with cecal involvement.
- Bowel perforation is an uncommon complication.
Differential diagnosis:
- Cavitary form : malignant stromal tumor or perforated colonic carcinoma.
- Bulky lymphomatoid masses are larger than the ones encountered in colorectal adenocarcinomas.
- In favor of the lymphoma diagnosis:
- Extension into the terminal ileum.
- Well-defined margins with preserved fat planes.
- Absence of involvement of adjacent structures.
- Perforation without any desmoplastic response.
4/ Pharynx
Non-Hodgkin’s lymphomas represent 10 to 15% of all pharyngeal malignant tumors.
It usually occurs in the palatine fossae,
nasopharynx,
and base of the tongue.
About 25% of patients with pharyngeal lymphoma have multiple sites of involvement.
Cervical lymph nodes are also involved in more than 50% of patients.
MRI is the reference imaging for the study of the pharynx; However,
CT patterns can include:
- Lobulated masses involving the palatine fossae or base of the tongue Fig. 17
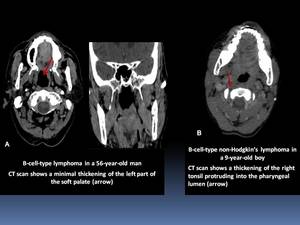
Fig. 17
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
- The overlying mucosa may have a coarse,
nodular appearance.
- Submucosal infiltration can obliterate normal anatomic landmarks of the pharynx Fig. 18
- It may be impossible to differentiate from pharyngeal carcinomas on the basis of radiographic criteria.
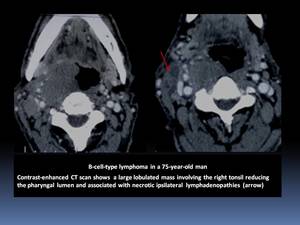
Fig. 18
References: Department of Radiology, Institute Salah Azaiez of Cancerology / Tunisia 2018.
5/ Oesophagus
The esophagus is the rarest site of GI lymphoma,
accounting for less than 1% of cases.
It occurs usually in patients with generalized lymphoma :
- Direct invasion of the esophagus by lymphomatous nodes in the mediastinum.
- Contiguous spread of lymphoma from the gastric fundus.
- Synchronous development of lymphoma in the esophageal wall.
- Rarely,
esophageal lymphoma can be primary.
CT findings can show:
- Extrinsic compression and mass effect on the esophagus with or without areas of ulceration.
- Thickened wall with narrowed lumen are nonspecific and may mimic esophageal adenocarcinoma.
- Occasionally,
lymphomatous infiltration of the submucosa may cause enlargement and tortuosity of the longitudinal folds,
mimicking the appearance of varices.
- Polypoid,
ulcerated mass or an irregular stricture are indistinguishable from an infiltrating carcinoma.

















