21 paediatric multitrauma patient was examined using split-bolus technique at Children Clinical University hospital of Riga,
Latvia,
from February 14,
2017 to April 14,
2017.
CT exams were performed with 4 different proportion of i/v contrast medium.
The patients were examined splitting the non-ionic iodine contrast medium iohexol of 300 mg I/ml or iodixanolumof 320 mgI/ml per dose of 1,2 ml/kg in two parts one of which was administered manually and after 7-10 minutes the other part was introduced through bolus injector system followed by scanning as the portovenous phase (with the delay of 50-60 seconds).
The patients were examined using 4 different proportions of administering the iodine contrast medium (2/3+1/3,
1/3 + 2/3,
1/4 + 3/4 and 1/5 + 4/5) divided in 4 groups depending on the used proportions of contrast medium – 2/3 of contrast medium,
followed by 1/3 of contrast medium.
The exams were performed with 64-slice scanner. After obtaining the topogram,
the bolus injector system was connected to the patient’s i/v cannula.
The first contrast media dose was administered manually,
and the second dose was administered via the bolus injector; the speed of contrast media injection depended on patient’s i/v cannula size and the experience of radiographer.
The performed CT exams were assessed by 3 experienced paediatric radiologists using a dedicated questionnaire grading the contrast of abdominal organs and structures as poor,
good or very good.
The results were processed and the graphs drawn by MS Excel.
With proportion 1/3 + 2/3 the gradation of majority of abdominal organs and structurs was poor or good.
Very good visualization was obtained in only 10% of cases (liver,
spleen,
kidneys and bladder) .
The proportion of bad contrast in many of abdominal structures showing bad contrast is quite obvious (Figure 1).
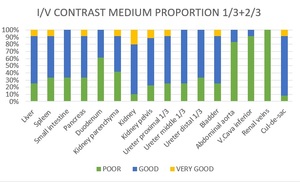
Fig. 1
Figure 1.
Visualization of abdominal organs and structures using proportion of the contrast medium 1/3+2/3.
With proportion of 1/4 + 3/4 very good contrast was obtained in almost 40% of abdominal structures and good contrast – in about 50% of organs.
With this proportion aorta and v.
cava inferior showed the highest rate of bad contrast – 30 and 20%,
respectively,
which is not clinically important since in case of children politrauma the damage of these structure occur exceptionally rarely.
No bad contrast was observed in liver,
spleen and kidneys which are the main risk organs of parenchymal rupture (Figure 2).
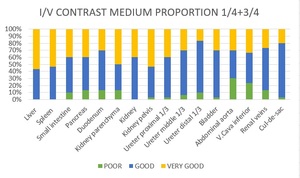
Fig. 2
Figure 2. Visualization of abdominal organs and structures using the proportion of the contrast medium 1/4+3/4
With proportionof 1/5 + 4/5 the majority of organs showed good contrast whereas very good contrast was obtained in only about 20% of all abdominal structures.
The amount of organs of „poor”contrast was relatively low,
but higher than in proportion 1/4 + 3/4 (Figure 3).
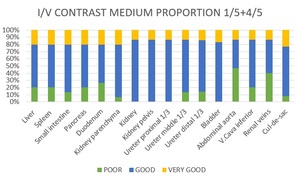
Fig. 3
Figure 3.
Visualization of abdominal organs and structures using the proportion of the contrast medium 1/5+4/5.
With proportion of 2/3 – 1/3 only kidneys,
ureter and bladder had very good contrast where as other abdominal organs and structures showed poor contrast (Figure 4).
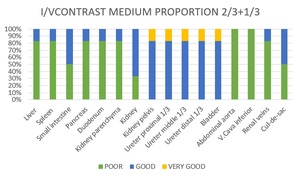
Fig. 4
Figure 4. Visualization of abdominal organs and structures using the proportion of the contrast medium 2/3+1/3.
Among all the politrauma patients included in the study there were cases of spleen and kidney rupture but no cases of liver or pancreas rupture were present.
Case Nr.
1.
6 y.o.
girl,
after a car accident,
suspected of perforation of the abdominal organs,
pancreas injury and bladder trauma.
Split bolus technique of 1/4+3/4 with i/v Visipaque 320 per dose of 1.2 ml/kg was applied injecting 8 ml manually ,
and after 10 minutes followed by 25 ml with bolus speed of 1.5 ml/sec.; the scan delay was 55 sec.
No injury was found.
Figures 5 and 6 show the good contrast of liver and spleen parenchyma,
the left kidney and the portal vein - figure 7 shows the renal excretory system.
Figure 8 shows the good contrast of the renal parenchyma with the excretory system in the coronary reconstruction image,
and figure 9 shows the renal excretory system in the volume rendering MIP image.
Figure 5. The very good contrast of the liver and spleen.
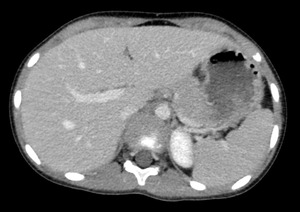
Fig. 5
Figure 6. The very good contrast of the liver,
spleen,
the left kidney as well as the portal vein.
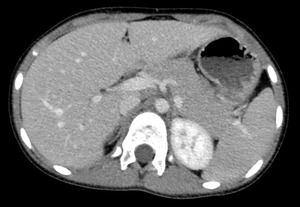
Fig. 6
Figure 7. The very good of the renal excretory system (bone window)

Fig. 7
.Figure 8. The good contrast of the renal excretory system
in the coronary reconstruction as well as volume rendering MIP image.

Fig. 8
Figure 9. The very good contrast of the renal excretory system in the volume rendering MIP image

Fig. 9
Case Nr.
2.
13 y.o.
girl,
after a car accident,
suspected of perforation of the abdominal organs
Splitt bolus technique of 1/4+3/4 with i/v Visipaque 320 per dose of 1.2 ml/kg was applied injecting 10 ml manually,
after 7 minutes followed by 30 ml with bolus speed of 2.0 ml/sec.; the scan delay was 60 sec.
The images shows splenic rupture of grade V with active bleedingand haemoperitoneum (Figures 10,
11 un 12).
Figure 10.
The splenic rupture with haemoperitoneum.
Note the good contrast of liver parenchyma as well as the very good contrast of the splenic parenchyma and its rupture.
The contrast medium extravasation is present.
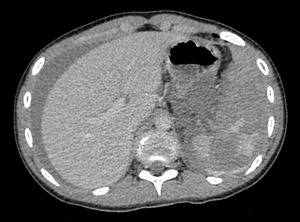
Fig. 10
Figure 11.
The splenic rupture with haemoperitoneum.
Note the very good contrast of the splenic parenchyma and its rupture as well as the contrast medium extravasation representing active bleeding.

Fig. 11
Figure 12.
The splenic rupture with haemoperitoneum.
Note the good contrast between the splenic rupture and parenchyma as well
as the site of active bleeding at the upper pole of the left kidney.

Fig. 12
Case Nr.
3.
10 y.o.
boy after a fall from a height of 2 m.
Split bolus technique of 1/4+3/4 with i/v Visipaque 320 per dose of 1.2 ml/kg
was applied injecting 7 ml manually,
and after 10 minutes followed by 50 ml with bolus speed of 2.0 ml/sec.
the scan delay was 55 sec.
The images showed laceration of the upper pole of spleen (Figures 13 and 14). Figure 13.
Laceration of the splenic upper pole.
Please note the good contrast of the liver parenchyma as well as between the splenic parenchyma and the ruptures.
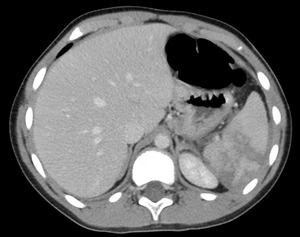
Fig. 13
Figure 14.
Laceration of the splenic upper pole,
coronary reconstruction.
Please note the good contrast between the splenic parenchyma and ruptures as well as the very good opacifation of the renal excretory system.

Fig. 14
Case Nr.
4.
15 y.o.boy – the follow-up CT examination after the accident being a scooter driver,
presenting with multiple abdominal trauma 15 days ago.
Now complaining of abdominal pain. Splitbolus technic of 1/4+3/4 with i/v Omnipaque 300 per dose of 1.2 ml/kg
was applied injecting 15 ml manually,
and after 10 minutes followes by 50 ml with bolus speed 2.0 ml/sec.;
the scan delay was 55 sec.
The images showed repeated splenic rupture,
subcapsular rupture of the left kidney and haemoperitoneum (Figures 15 and 16.)
Figure 15.
The splenic rupture with haemoperitoneum.
Please note the good contrast of liver parenchyma and very good contrast of parenchyma of the right kidney.

Fig. 15
Figure 16.
Rupture of the lower pole of left kidney with no damage of the renal excretory system.
Please note the very good contrast of the kidney parenchyma as well as the very good contrast between the rupture and the parenchyma as well as between the good opacifation of the renal excretory system.
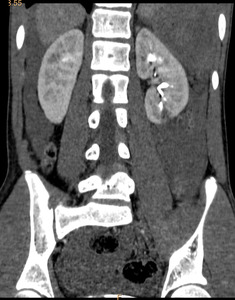
Fig. 16

