ECR 2018 / C-3087
Folds and spaces: a pictorial review of peritoneal anatomy and pathology
Congress:
ECR 2018
Poster Number:
C-3087
Type:
Educational Exhibit
Keywords:
Abdomen, Anatomy, CT, Education, Education and training
Authors:
F. M. F. Gomes1, C. A. B. Oliveira2, F. D. S. Costeira2, C. Esteves2, V. Mendes2, P. F. R. Oliveira da Silva2; 1Guimarães/PT, 2Braga/PT
DOI:
10.1594/ecr2018/C-3087
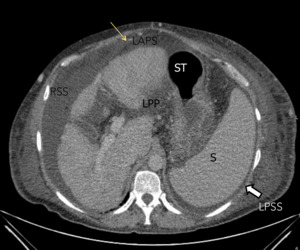
 which is outlined by ascites in this patient with chronic hepatopathy. There is fluid in the left anterior perihepatic space (LAPS) and in the right subphrenic space (RSS), which are separated by the falciform ligament.
The left posterior perihepatic space (LPP) lies parallel to the lesser curvature of the stomach (ST), and it is limited posteriorly and on the right by the gastrohepatic ligament (not showed).
L, Liver; RSP, right subphrenic space; LPSS, left posterior subphrenic space; ST, stomach; .S, Spleen; LPP, Left posterior perihepatic space. References: Hospital de Braga, Portugal")
Fig. 1:
Axial CT image, obtained in a 55-year-old man shows the falciform ligament...
.
The right subphrenic space (RSS) communicates with the right percolic space (RC) and the right subhepatic space (arrow). References: Hospital de Braga, Portugal")
Fig. 2:
Coronal CT image in a 66-years-old man shows the right subhepatic space or...
 and axial (B) CT image shows the superior (LSs) and inferior (LSi) recesses of the lesser sac in the supramesocolic space. References: Hospital de Braga, Portugal")
Fig. 3:
Coronal (A) and axial (B) CT image shows the superior (LSs) and inferior (LSi)...
. Axial CT image, obtained in a 55-year-old man shows the falciform ligament (yellow arrow) which is outlined by ascites in this patient with chronic hepatopathy. The left posterior perihepatic space (LPP) lies parallel to the lesser curvature of the stomach (ST), and it is limited posteriorly and on the right by the gastrohepatic ligament (not showed).
The left posterior subphrenic (or perisplenic) (LPSS) space surrounds the spleen.
L, Liver; RSP, right subphrenic space; LPSS, left posterior subphrenic space; ST, stomach; S, Spleen. References: Hospital de Braga, Portugal")
Fig. 4:
The left anterior perihepatic space (LAPS). Axial CT image, obtained in a...
 lies between the stomach and the diaphragm. This space extends posteriorly and communicates with the posterior subphrenic (or perisplenic) space, which surrounds the spleen (S). References: Hospital de Braga, Portugal")
Fig. 5:
The left anterior subphrenic space (LASS) lies between the stomach and the...
, which contains the short gastric vessels. References: Hospital de Braga, Portugal")
Fig. 6:
Coronal CT image of the upper abdomen, obtained in a 53-year-old man, shows...
. References: Hospital de Braga, Portugal")
Fig. 7:
Coronal CT image of the upper abdomen, obtained in a 63-year-old man, shows...
. References: Hospital de Braga, Portugal")
Fig. 8:
Phrenicocolic ligament (yellow arrow).
 and in the right subphrenic space (RSS), which are separated by the falciform ligament (yellow arrow). References: Hospital de Braga, Portugal")
Fig. 9:
Axial CT shows fluid in the left anterior perihepatic space (LAPS) and in the...

Fig. 10:
Lateral to the ascending and descending colon are the right and left paracolic...
 in females (asterisk).
Anteriorly, the medial umbilical fold (yellow arrow), which contain the obliterated umbilical arteries, divide the paravesical space, into lateral (inguinal fossae) and medial (supravesical fossae) compartments. The inguinal spaces are further subdivided into medial and lateral inguinal fossae, by the lateral umbilical folds (blue arrows), which contains the inferior epigastric artery, corresponding to the sites of indirect and direct inguinal hernias, respectively. References: Hospital de Braga, Portugal")
Fig. 11:
In the pelvis, the peritoneum reflects over the pelvic organs, creating the...
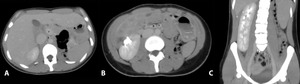
 Axial CT of a 7-year-old girl. Axial contrast-enhanced CT scan obtained at the level of the upper abdomen shows an inverted relationship between superior mesenteric artery (a) and superior mesenteric vein (v).
B) Contrast-enhanced CT at a level below.
C) Coronal contrast-enhanced CT shows the presence of a crossed fused renal ectopia referring to an anomaly where the kidneys are fused and located on the same side of the midline (right). References: Hospital de Braga, Portugal")
Fig. 12:
A) Axial CT of a 7-year-old girl. Axial contrast-enhanced CT scan obtained at...
. Contrast-enhanced CT image shows a dilated and stool-filled cecum located in the left upper quadrant. This appearance results from twisted collapsed bowel with enhancing engorged vessels radiating from the twisted bowel. References: Hospital de Braga, Portugal")
Fig. 13:
The “whirl sign” of cecal volvulus (blue arrow). Contrast-enhanced CT image...

Fig. 14:
A 64-year-old man with abdominal pain. CT image showed a clustered dilated...
 and tiny nodes (asterisk). References: Hospital de Braga, Portugal")
Fig. 15:
A 65-year-old man with mesenteric panniculitis. Axial contrast-enhanced CT...
. References: Hospital de Braga, Portugal")
Fig. 16:
A 67-year-old man with omental infarction. Contrast-enhanced CT performed for...

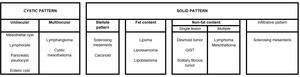
Table 1:
Mesenteric neoplasms.
 and ascites caused by metastases from colon cancer. References: Hospital de Braga, Portugal")
Fig. 17:
Contrast-enhanced abdominal CT scan shows omental thickening (arrows) and...
 calcifications consistent with Pseudomyxoma Peritonei. References: Hospital de Braga, Portugal")
Fig. 18:
Pseudomyxoma Peritonei. Contrast-enhanced TC showing low attenuation fluid...
, posterior renal fascia (green arrow), lateroconal plane (blue arrow). K, kidney. References: Hospital de Braga, Portugal")
Fig. 19:
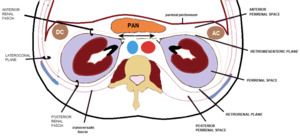
Main retroperitoneal fascias: anterior renal fascia (yellow arrow), posterior...
. References: Hospital de Braga, Portugal")
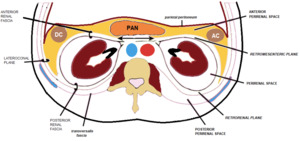
Fig. 20:
Representation of the retroperitoneal cavity - anterior pararenal space...
. References: Hospital de Braga, Portugal")
Fig. 21:
Representation of the retroperitoneal cavity - perirenal space (purple).
. References: Hospital de Braga, Portugal")
Fig. 22:
Representation of the retroperitoneal cavity - posterior pararenal space (pink).
. References: Hospital de Braga, Portugal")
Fig. 23:
Typical “molar tooth” configuration of a prevesical fluid collection (red...