To understand the radiographic image,
first we have to understand some basic physics.
X-rays travel in straight lines,
leaving the X-ray tube,
as a beam of X-rays diverging.
The structures the X-rays hits first will be magnified in the image,
in relation to those which are nearer the detector.
To reduce magnification the X-ray source can be moved further away from the subject.
Structures that need to be measured accurately should be placed closer to the detector.
These are the reasons why posteroanterior (PA) incidence is the more indicated to study the chest,
avoiding mediastinum magnification.
The terms posterior and anterior refer to the direction of the x-ray beam through the thorax.
This is how the different chest X-ray incidences are acquired:
PA – patient is standing up facing the upright image receptor.
The superior aspect of the receptor should be 5 cm above the shoulder joints,
the chin raised as to be out of the image field and shoulders rotated anteriorly to allow the scapulae to move laterally off the lung fields.
Anteroposterior (AP) – patient is upright as possible with their back against the image receptor.
The chin should be raised as to be out of the image field,
hands placed by the patient's side and shoulders depressed to move the clavicles below the lung apices.
Lateral view – patient is standing up with the left side of the thorax adjacent to the receptor.
Both arms should be raised above the head to prevent superimposition,
and the chin raised as to be out of the image field.
Apical view – it is an AP view with patient standing up,
where midcoronal body plane and image receptor should form a 45 angle degree.
This position can be achieved standing with feet approximately 30cm away from the image receptor,
with back arched until upper back,
shoulders and head are against the image receptor.

Fig. 1: Medical radiographic image - chest X-ray study.
References: Department of Radiology, Algarve Hospital and University Centre, Portimão/Portugal 2018
Medical radiographic image,
as so the chest X-ray,
is the result of interaction between the the X-ray beam and the human body.
Some X-rays pass freely through the body and the others are variably attenuated by anatomical structures – absorbed/scattered.
When an X-ray reach the receptor,
after not being totally absorbed/scattered,
will “burn” the film and appear at the image as a dark spot.
The reverse also happens,
the denser the tissue,
more X-rays are attenuated or totally absorbed by the body part,
so less X-ray will reach the receptor and the final image will appear whiter.
Classically,
five densities are described at radiographic images,
from darker→whiter/less dense→most dense:
Air → Fat → Soft tissue → Bone → Metal
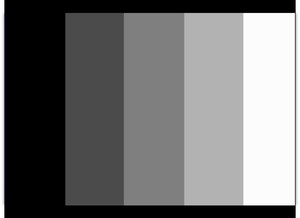
Fig. 2: Radiographic densities grey scale: Air → Fat → Soft tissue → Bone → Metal.
References: Department of Radiology, Algarve Hospital and University Centre, Portimão/Portugal 2018
Contrast within the overall image depends on differences in both the density and thickness of body structures.
The greater the differences between two adjacent structures,
the greater contrast.
Chest X-ray role has changed over the years,
especially with introduction and evolution of CT.
Nevertheless,
it remains a major screening,
diagnosis and follow-up tool.
With so many and developed imaging techniques,
younger radiologists are less focused and less confident in evaluating and reporting conventional radiology,
in benefit of US,
CT and MRI learning.
The following checklist is just a start to initiate chest X-ray reading exercise,
in a structured way,
creating solid basis for continuous learning.
