The CT findings of abdominal tuberculosis are frequently related to caseous necrosis,
which is the hallmark of this disease.
However,
depending on the involved organ,
tuberculous lesions can mimic other diseases - both neoplastic and non-neoplastic - such as lymphoma,
leukemia,
metastasis,
sarcoidosis,
histoplasmosis or pyogenic infections.
Although a positive culture or histologic analysis of biopsy specimens are still required in many patients to yield the definitive diagnosis,
recognition and understanding the spectrum of imaging features of abdominal tuberculosis can aid in establishing the diagnosis.
The most common sites of tuberculosis in the abdomen,
in descending order of frequency,
are lymph nodes,
genitourinary tract,
peritoneal cavity,
and gastrointestinal tract.
Tuberculous involvement of the liver,
spleen,
pancreas,
and adrenals is rare,
but more common in disseminated disease.
TUBERCULOUS LYMPHADENITIS
Lymphadenopathy is the most common manifestation of abdominal tuberculosis and accounts for 20% of extrapulmonary infection,
either seen in isolation or with other organ involvement.
Periportal,
peripancreatic,
mesenteric,
omental and upper para-aortic nodes are frequently affected.
Tuberculous involvement of lower para-aortic nodes is uncommon except in disseminated tuberculosis.
Lymphadenopathy in CT images is usually seen as enlarged and/or confluent lymph nodes,
with a hypoattenuating center and variable enhancement patterns,
being the peripheral enhancement the most common (caseous necrosis).
This kind of enhancement is highly suggestive of TB,
although similar lesions may be found in lymphoma,
metastases and Whipple disease.
Others imaging patterns are defined as clusters of nodes or conglomerate nodal masses with mixed or homogeneous attenuation.
Following the treatment or healing,
these nodes can calcify.
Lymphoma is more likely to affect upper and lower para-aortic nodes,
and the nodes are often larger than tuberculous lymphadenitis.
In the presence of a known primary malignancy,
enlarged abdominal nodes are more likely to be nodal metastases.
The secondary gastro-intestinal,
urinary and biliary obstruction is rarely seen,
despite the development of masses due to confluent lymphadenopathy.
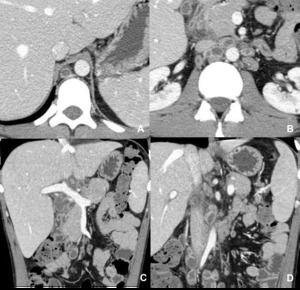
Fig. 1: Tuberculous lymphadenitis. Necrotic lymph nodes in the retrocrural space, lumboaortic chain and peripancreatic region.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
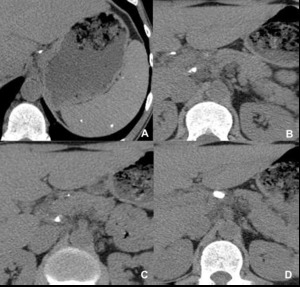
Fig. 2: Tuberculous lymphadenitis (residual disease). Small calcified splenic granulomas and peri-pancreatic calcified adenopathies, in a patient with a history of splenic and lymph nodes tuberculosis.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
URINARY TRACT TUBERCULOSIS
The genitourinary tuberculosis is the most common manifestation of extrapulmonary tuberculosis,
accounting for 4-17% of extrapulmonary infection.
The upper renal tract is the most frequently affected part of the genitourinary tract.
Urinary tract tuberculosis can be associated with increased urinary frequency,
pain,
haematuria and sterile pyuria.
- Renal Tuberculosis
The earliest change is the “moth-eaten” calix at intravenous urography,
which progresses to papillary necrosis,
that appears as small poorly marginated areas of reduced enhancement at the tip of the medullary pyramids.
Others alterations may be seen,
like focal caliectasis or uneven caliectasis related to an infundibular strictures and generalized hydronephrosis due to a stricture of the ureteropelvic junction (Kerr kink).
Renal parenchymal involvement can appear as: focal nephritis - wedge-shaped areas of reduced enhancement that is identical in appearance to nephritis caused by other organisms; nodular mass (tuberculoma) - an uncommon appearance that can be mistaken for a tumour; or parenchymal scar formation and calcification - can develop following healing by fibrosis.
The end-stage fibrosis and subsequent obstructive uropathy produce autonephrectomy,
with characteristic calcifications in a lobar distribution.
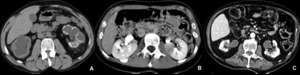
Fig. 3: Renal tuberculosis. A, Bilateral caliectasias due to pyelic stenosis, with calcifications in the left collecting system. There is a reduction in parenchymal thickness. B, Hypodense nodular lesion in the left kidney of a patient with pulmonary tuberculosis, compatible with renal tuberculoma. C, Multiple parenchymal defects, mainly in the left kidney, due to previous renal tuberculosis.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
- Ureteral tuberculosis
Dilatation and a ragged irregular appearance of the urothelium are the first signs of ureteral tuberculosis,
being that the distal third of the ureter is the most commonly involved.
Advanced ureteral fibrosis owing to multiple strictures and mural calcification may be seen.
Strictures have a predilection for anatomic narrowing points: at the pelviureteric junction,
across the pelvic brim and at the vesicoureteric junction.

Fig. 4: Ureteral tuberculosis. Signs of right uretero-hydronephrosis due to stenosis of the distal third of the homolateral ureter.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
- Bladder tuberculosis
Tuberculous cystitis appears as focal or global wall thickening.
In long-term disease,
the bladder is small and irregular due to scarring and calcifications.

Fig. 5: Bladder tuberculosis. The bladder is small and irregular due to scarring and calcifications in a patient with chronic tuberculous cystitis.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
TUBERCULOUS PERITONITIS
Tuberculous peritonitis accounts for 2% of extrapulmonary infection.
Three CT patterns of peritoneal involvement have been described: wet type (90%) - characterized by large amount of free or loculate ascites,
seen in most patients; fibrotic-fixed type (7%) - characterized by matted bowel loops and mesentery,
omental mass and small volume ascites; and dry type (3%) - characterized by mesenteric thickening,
fibrous adhesions and caseous nodules.
Ascites can have high attenuation due to its high protein or cellular content.
Smooth thickening and strong contrast enhancement of the parietal peritoneum is typically seen with tuberculous peritonitis.
Peritoneal irregular thickening and enhancement associated with nodular implants are uncommon and are more suggestive of peritoneal carcinomatosis.
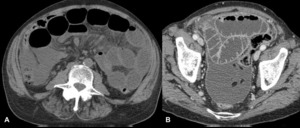
Fig. 6: Tuberculous peritonitis. Male patient, 77 years old, with intestinal occlusion due to tuberculosis. The CT study shows infiltration of the mesentery (sign of the starry mesentery) and peritoneal effusion, associated with thickening and enhancement of the peritoneum, compatible with tuberculous peritonitis (ascitic-wet type).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
GASTROINTESTINAL TRACT TUBERCULOSIS
Tuberculosis of the gastrointestinal tract is relatively uncommon.
Gastrointestinal tuberculosis can present with abdominal pain,
abdominal mass,
vomiting,
diarrhoea,
dysphagia and gastrointestinal bleeding.
The most common sites of disease are the caecum and distal ileum,
seen in 80%–90% of patients with abdominal tuberculosis.
Other GI segments,
for example the colon (9%) and duodenum (2%),
are only rarely involved.
Intestinal tuberculosis has three main forms: ulcerative – shallow ulcers with fold thickening; hypertrophic – more prominent mural thickening with inflammation extending into adjacent tissues,
like an exophytic mass around the ulcerated lumen; and fibrosing – strictures that can cause obstruction.
Classical shallow tuberculous ulcers with elevated margins are more clearly visualized with double-contrast barium studies because of increased mucosal detail.
CT may show the characteristic appearance of asymetric thickening and gaping of the ileocaecal valve (incompetent) and circumferential wall thickening of terminal ileum and caecum.
In advanced disease,
characteristic deformities include symmetric annular “napkin ring” stenoses and obstruction,
shortening,
retraction,
and pouch formation.
That can also mimic carcinoma,
but cecal carcinoma rarely extends beyond the ileocecal valve.
Perforation and fistulae are reported to occur in approximately 5% of patients,
with haemorrhage and malabsorbtion syndrome also described.
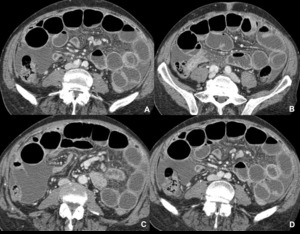
Fig. 7: Gastrointestinal tuberculosis. Wall thickening of the terminal ileum and cecum, causing luminal stenosis with dilatation of the upstream small bowel.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
HEPATOSPLENIC TUBERCULOSIS
Hepatosplenic tuberculosis is an uncommon antemortem diagnosis,
usually seen in disseminated tuberculosis.
The patients typically present abdominal pain and hepatosplenomegaly.
Jaundice can occur in the absence of biliary tract involvement.
The patterns of hepatosplenic tuberculosis include micronodular (miliary) and macronodular (tuberculoma) forms.
The micronodular form usually occurs in association with military pulmonary tuberculosis,
consisting of innumerable tiny low attenuation foci on CT.
The macronodular form is rare and consists of one or more low attenuation masses with irregular ill-defined margins and minimal enhancement in a diffusely enlarged liver or spleen.
These lesions are called tuberculomas and may calcify forming calcified granulomas.
The miliary pattern of disease can be mistaken for fungal abscesses,
metastases and sarcoidosis.
The macronodular pattern can be mistaken for pyogenic abscesses,
metastases and primary malignant tumor.
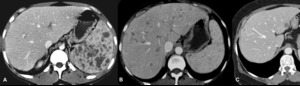
Fig. 8: Hepatosplenic tuberculosis. Immunosuppressed patients with simultaneous pulmonary tuberculosis. A, Mixed pattern. B, Miliary pattern. C, Macronodular pattern.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 9: Hepatic and adrenal tuberculosis (residual disease). Calcified granulomas in the liver and left adrenal gland.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
PANCREATIC TUBERCULOSIS
Tuberculosis of the pancreas is rare.
The pancreatic body,
head,
and tail are involved in descending order of frequency.
Pancreatic tuberculosis can appear as one or more hypoattenuating masses of variable sizes that show rim contrast enhancement,
or rarely,
as a diffusely enlarged pancreas.
Absence of pancreatic duct dilatation or vascular invasion and necrotic lymphadenopathy are all together highly suggestive of TB,
differentiating from pancreatic adenocarcinoma or chronic pancreatitis.
ADRENAL TUBERCULOSIS
Adrenal tuberculosis is seen in up to 6% of patients with active tuberculosis.
It almost always appears as bilateral masses with or without central low attenuation and rim enhancement.
Bilateral adrenal masses can be mistaken for metastases,
adenomas or lymphoma.
The gland may undergo atrophy and calcification in the end stage of disease.
The Addison’s syndrome can occur when more than 90% of the adrenal tissue is destroyed.

Fig. 10: Adrenal tuberculosis (residual disease). Calcified granulomas in the left adrenal gland.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 11: Adrenal tuberculosis. Mass in the left adrenal gland with heterogeneous enhancement due to the presence of areas of necrosis, in an immunosuppressed patient with cerebral tuberculomas.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT


. Small calcified splenic granulomas and peri-pancreatic calcified adenopathies, in a patient with a history of splenic and lymph nodes tuberculosis. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")



 and peritoneal effusion, associated with thickening and enhancement of the peritoneum, compatible with tuberculous peritonitis (ascitic-wet type).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT")


. Calcified granulomas in the liver and left adrenal gland.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
. Calcified granulomas in the left adrenal gland. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
