Temporal bone is formed by tympanic,
squamous and petrous portions. Several fissures may be identified in the limits of the three portions.
The most relevant of them is the tympanosquamous fissure located between mandibular fossa and posterior zygomatic tubercle.
Its medial extreme is divided by the inferior projection of the tegmen tympani.
The anterior division constitutes the petrosquamous fissure and the posterior is the petroympanic.
(PTF) (fig 1)
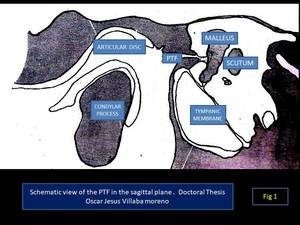
Fig. 1: Schematic view of the PTF in the sagittal plane
References: Oscar jesus Villalba Moreno
The PTF transmits the discomalleolar ligament (DML),
the anterior ligament of malleus (ALM),
the chorda tympani and the posteromedial branches of anterior tympanic artery.
The two ligamentous structures originate in the neck of malleus and its anterior process.
They are closely related with temporomandibular joint (TMJ) and cross the PTF independently through the canal of Hughier that is divided in two by a small bone septum located inferiorly.
The DML presents a triangular shape and is located medially.
It inserts in the posterior capsule and meniscus of TMJ.
The ALM is rounded and located laterally.
It runs through the Hughier canal accompanied by the chorda tympani.
Part of ALM fibers adhere to the margin of PTF and the sphenoid spine and a relevant portion of its fibers are continuous with esfenomandibular ligament and in consequence,
can be considered as the intratympanic portion of malleomandibular ligament.( fig 2 ).
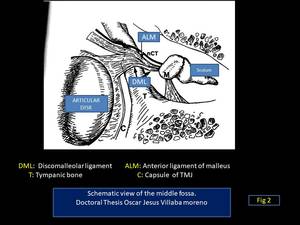
Fig. 2: Schematic view of the middle fossa
References: Oscar jesus Villalba Moreno
The existence of these two otomandibular ligaments constitutes a true mechanical connection between the mandible and TMJ structures and the middle ear.
In addition,
the petrotympanic fissure constitutes a way of communication between middle ear and TMJ that facilitates the propagation of infections or inflammatory processes between the two structures.
The degree of ossification and the size of the petrotympanic fissure are variable between subjects.
Sato and cols classified the PTF in three different types according with its morphology in the sagittal plane (Fig 3-6).
The type 1 consists in a wide tunnel shaped structure.
Type 2 was a tunnel-shaped structure widely open in the entrance of the petrotympanic fissure to the mandibular fossa and gradually thinning out in the tympanic cavity.
Finally the type 3 morphology was a tunnel shaped structure widely open in the entrance of the mandibular fossa followed by a middle region with flat-shaped tunnel structure and a narrow exit in the tympanic cavity.
In axial plane the morphology of three typologies also differed between tunnel-like structure (type 1),
wide slit structure (type 2) and narrow slit structure (type 3).
The maximum communication between TMJ and middle ear occurs in cases of type 1 PTF.
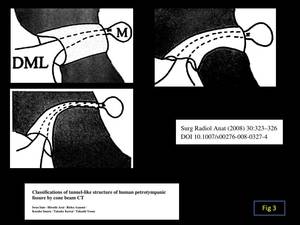
Fig. 3
References: Oscar jesus Villalba Moreno
Fig. 4 Fig. 5 Fig. 6
This work sought to investigate the variable morphology of PTF in human cadaveric specimens using anatomic sectioning and helical CT images and to correlate the measurements obtained with both approaches in order to validate the usefulness of helical CT to further investigate the morphology of PTF in living subjects.
Anatomic blocs (n=15) containing the temporal bone and TMJ were used for this study.
Blocs were collected from 15 human bodies donated to the Faculty of Medicine of Universitat Autònoma de Barcelona.
(Fig 7)
The specimens were from male (46.7%) and female cadavers (53.3%) and from the right (46.7%) and left (53.3%) sides.
The age of the specimens (mean±SD) was 78.9±4.2 years.
Tomographic images of the specimens were obtained with a helical scanner of 16 detector rows (Siemens Somatom Sensation 16,
Siemens Forchheim,
Germany.
The protocol for exploration of inner ear (INNER EAR VOL) was used in all the cases and the acquisition included the whole specimen.
DICOM images were visualized with ORS visual software 1.5.1 (Object Research Systems Inc.
Montreal,
Canada).
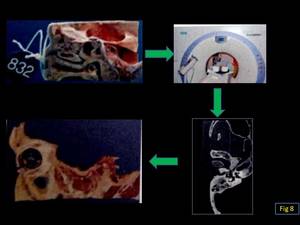
Fig. 8
References: Oscar jesus Villalba Moreno
Specimens were frozen and sectioned in the sagittal plane.
Parasagittal sections were obtained starting from the medial plane and progressing laterally.
The thickness of the sections was between a minimum of 3 and a maximum of 6 mm depending on the specimen..
Obtained sections were rinsed in tap water and those representatives of PTF were selected for morphological determinations
The following variables were measured both in anatomic sections and radiologic images at the level of sagittal plane
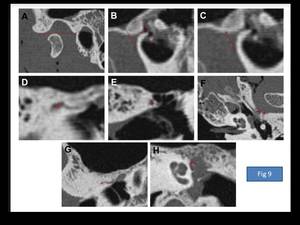
Fig. 9
References: Oscar jesus Villalba Moreno
Longitude of mandibular fossa (L-MF)
Longitude of PTF (L-PTF):
Vertical diameter of PTF at the level of mandibular fossa (VD of PTF-MF):
The following variables were determined only in radiologic images:
Vertical diameter of PTF at midpoint (VD of PTF-1/2):
Vertical diameter of PTF at the level of tympanic cavity (VD of PTF-TC):
Width of PTF at the level of mandibular fossa (W of PTF-MF):
Width of PTF at its midpoint (W of PTF-1/2):
Width of PTF at the level of tympanic cavity (W of PTF-TC):
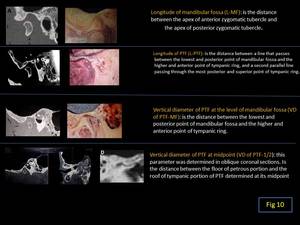
Fig. 10
References: Oscar jesus Villalba Moreno
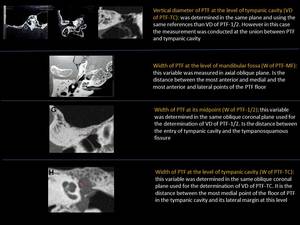
Fig. 11
References: Oscar jesus Villalba Moreno
Anatomic variables were determined twice by a single rater.
Radiologic variables were determined twice by two independent raters.
Statistical analysis
Bland-Altman plots were drafted to analyze the degree of agreement between the measurements made in anatomical sections and CT images.
To determine if any difference between measurement means was statistically significant,
calculated differences between means were statistically compared against the hypothetical value of zero.
Inter-rater agreement was investigated for all CT parameters by calculating ICC.
Differences between Sato’s three PTF morphologies were analyzed by one-way analysis of variance (ANOVA),
with Tukey’s multiple comparison test performed post hoc.
For all tests,
a two-tailed p < 0.05 was considered statistically significant.









