Anatomical sections
PTF was identified in all specimens located within the posteromedial region of the mandibular fossa.
In the sagittal plane,
it consisted of a thin communication between the retrodiscal region of the TMJ and the epitympanum.
The PTF had a descending trajectory and three segments that could be distinguished.
The anterior segment,
in contact with the TMJ,
was the widest of the three.
The posterior segment was the opening into the tympanic cavity,
and was narrowest.
Between these,
the middle segment was where the osseous walls of the PTF approximated.
MDCT evaluation
In the axial plane,
the PTF is difficult to visualize completely,
typically having a thin sinuous appearance.
In contrast,
the axial oblique plane enables visualization of the communication between the middle ear and mandibular fossa.
In all cases,
the PTF was divided,
by a thin septum,
into two canals: one lateral for the DML,
the other medial,
for the AML and chorda tympani.
In the sagittal plane,
the PTF’s morphology was identical to that observed in the anatomical sections.
By radiological morphology,
20% of the specimens were classified as Sato type 1,
46.7% as Sato type 2,
and 33.3% as Sato type 3.
In the coronal plane,
the PTF was not identified in any specimen.
However,
in coronal oblique images,
the PTF could be identified as a sinuous structure.
Morphometric variables
In the anatomical sections,
the length of the mandibular fossa was 16.8±0.9 mm (mean±SD) and the length of the PTF 4.7±0.7 mm.
The vertical diameter of this structure at the level of the mandibular fossa was 3.5±0.6 mm.
In the radiological images,
corresponding values were 17.4±0.7 mm,
5.3±0.8 mm,
and 4.0±0.7,
respectively.
Values obtained for the additional variables only measured on coronal oblique reformatted images were 0.7±0.3 mm for the vertical diameter at the midpoint of the PTF,
and 0.9±0.3 mm for the vertical diameter of the PTF at the tympanic cavity level.
The width or lateral diameter of the PTF at the level of the mandibular fossa determined in axial oblique radiological images was 7.7±0.6 mm.
Lateral diameters of the PTF at its midpoint and at tympanic level were 4.98±0.9 mm and 1.8±0.5 mm,
respectively.
On Bland-Altman plots,
measurements obtained for anatomical sections were significantly less than corresponding measurement made using the radiological images The difference in measurements between the anatomical sections and CT images was -0.55 mm for the L-MF,
-0.72 mm for the L-PTF,
and -0.53 mm for the VD of the PTF-MF.
For these three measurements,
the difference between the anatomical and radiological determinations was statistically different than the hypothetical value of zero.
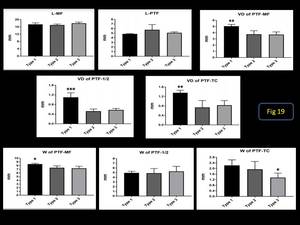
Fig. 13
References: Oscar jesus Villalba Moreno
In the radiological images,
some of the measurements differed between the three Sato types.
The variable vertical diameter of the PTF at the mandibular fossa level was significantly greater for type 1 (p=0.004) than types 2 and 3.
There were no significant differences in this parameter between type 2 and 3 specimens.
The same result was observed for the variables’ vertical diameter at the PTF midpoint (p<0.001) and tympanic cavity level (p=0.009).
The PTF type 1 specimens also were significantly wider at the mandibular fossa level (p=0.015) than types 2 and 3,
which again were not statistically different from each other.
The width at the tympanic cavity level was less among type 3 specimens (p=0.049) than the other two morphologies.
The PTF has also been proposed as a route for the propagation of middle ear infections to the TMJ,
both in infants and adults (Jain et al.
2008; Erol et al.
2006).
In the opposite direction,
the PTF may enable the spread of inflammatory processes from the TMJ to the middle ear,
causing serous otitis (Orhan et al.
2005; Scolozzi et al.
2004; Youniss 1991; Marasa and Ham 1988).
The clinical relevance of the PTF as a route of pathology propagation is broadly accepted and supported by several previously-published studies.
Our results indicate that,
even at an advanced age,
the PTF is universally present,
continuing to be a true anatomical communication between the middle ear and TMJ.



