· Pathology
UIP,
the radiologic and also pathologic pattern of IPF,
is caractherized by scattered fibroblastic foci with heterogeneous distribution that alternate interstitial inflammation and honeycombing.
These findings coexist with normal lung areas.
· Imaging findings:
Chest x-ray:
Imaging findings on a chest X-ray are not specific,
even though reticular pattern and bronchiectasis,
with lower lobes and costophrenic angles predominance are generally recognised. Fig. 1
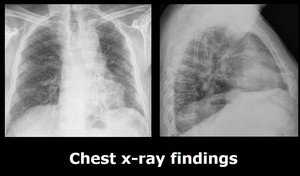
Fig. 1: Frontal and lateral chest x-ray show diffuse gross reticular pattern in a patient with IPF.
References: Department of Radiology, University Hospital Santa Lucía
MSCT (multi-slice CT):
High-quality CT images are essential.
Chest CT requires thin sections (<2 mm) and high spatial resolution reconstruction.
Images should be obtained at full inspiration to total lung capacity to avoid misinterpretation of key findings (eg,
ground glass opacity and fine reticulation).
Image findings:
- Honeycombing: it is considered the most specific sign of UIP.
It consists of a cluster of two or more layers of cystic air spaces,
usually with a diameter of 3–10 mm,
in the subpleural region. Fig. 2
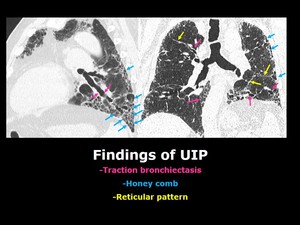
Fig. 2: Typical Findings of UIP.
References: Department of Radiology, University Hospital Santa Lucía
- Reticular pattern: On CT scans from patients with UIP,
reticulation is often irregularly spaced,
with a mixture of thick and thin lines. Fig. 2
Fig. 2: Typical Findings of UIP.
References: Department of Radiology, University Hospital Santa Lucía
- Traction bronchiectasis: This feature represents bronchial and bronchiolar dilatation caused by retractile fibrosis in the surrounding lung parenchyma.
In patients with UIP,
traction bronchiectasis are predominantly seen in the periphery of the lungs,
and affected airways typically have an irregular varicose appearance. Fig. 2
Fig. 2: Typical Findings of UIP.
References: Department of Radiology, University Hospital Santa Lucía
- Ground glass opacities: Many patients with fibrotic lung disease have ground glass opacities admixed with reticular abnormality or traction bronchiectasis,
that is,
ground glass opacities of interstitial origin.
Pure ground glass opacities,
that is,
of alveolar nature,
are not a feature of UIP,
even though they can be seen in non-fibrotic areas of the lung in acute exacerbation or infection.
- Emphysema: patients with IPF are almost invariably smokers,
and therefore,
usually have emphysema.
It is important for the radiologist to describe the extent of pulmonary emphysema,
since its influences the treatment and prognosis.
- There is mediastinal lymph node enlargement in up to 70% patients,
and it tends to affect the paratracheal regions. Fig. 3
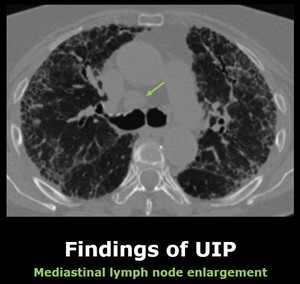
Fig. 3: Enlargment of a lower paratracheal right lymph node in a patient with UIP (arrow).
References: Department of Radiology, University Hospital Santa Lucía
· Diagnostic cathegories:
1. Typical UIP pattern Fig. 4
a.Basal and subpleural predominance
b.Reticular pattern with associated traction bronchiectasias
c.
Honeycombing
d.
Absence of features listed as inconsistent with a UIP pattern
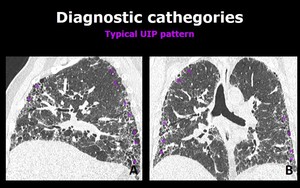
Fig. 4: Sagital (A) and coronal (B) chest CT scans show reticulation (arrows), traction bronchiectasis (arrowheads) and honeycombing (*) with a heterogeneous distribution but basal and subpleural predominance. These findings are consistent with a typical UIP pattern.
References: Department of Radiology, University Hospital Santa Lucía
2.
Probable UIP pattern Fig. 5
a.Basal and subpleural predominance
b.Reticular pattern with or without traction bronchiectasias
c.
Absence of features listed as inconsistent with a UIP pattern
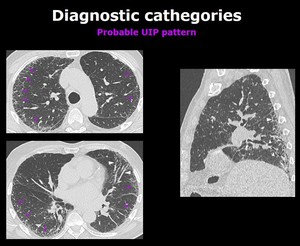
Fig. 5: Axial and sagital chest CT images show a reticular pattern (arrows) and traction bronchiectasis (arrowheads) with subpleural and basal predominance. There is also absence of honeycombing. All of these findings are consistent with a Probable UIP pattern.
References: Department of Radiology, University Hospital Santa Lucía
3.
Most consistent with non- UIP pattern Fig. 6
a.
Upper or mid-lung predominance
b.
Peribronchiovascular predominance
c.
Extensive ground-glass abnormality
d.
Profuse micronodules
e.
Discrete cysts
f. Diffuse mosaic attenuation/air-trapping
g.
Parenchymal consolidations
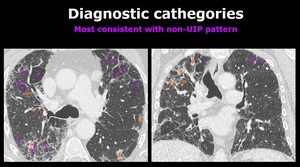
Fig. 6: Axial and coronal chest CT images show reticulation (purple arrows) , traction bronchiolectasis (orange arrows), ground glass opacities (orange *) and air trapping (*). These findings are bilateral and asymmetrical and have an upper lobe predominance.
References: Department of Radiology, University Hospital Santa Lucía
Diagnostic management
When there is suspicion of an interstitial lung disease,
a high-resolution CT scan of the chest should be obtained to determine whether the disease is present and to identify specific radiologic patterns.
Once interstitial lung disease has been identified,
a history and physical examination focused to identify disorders that cause interstitial lung disease (ILD),
should be done.
Clinical checklist for disorders associated with ILD
-Severity,
duration,
and pace of the primary respiratory symptoms.
-Symptoms or signs of a systemic autoimmune disorder.
-Exposure to inhaled antigen (pets,
birds,
home and work environment…) and temporal association between the exposure and symptom onset.
-Occupational disease.
If no cause can be identified,
IPF should be included in the differential diagnosis,
particularly for patients who are more than 50 years of age.
The presence of a typical or probable UIP pattern on CT provides a diagnosis of IPF in the appropriate clinical context.
If clinical and imaging data are not diagnostic,
a lung biopsy should be considered if the results are expected to influence therapy.
Biopsy samples should be taken from multiple lobes,
and the most severely affected areas should avoid sampling,
they typically show advanced,
nondiagnostic fibrosis.
· Differential diagnosis
The radiological UIP pattern can be sometimes difficult to diagnose due to its resemblance with other entities.
We discuss some of diseases that may mimic them,
and the features that help differenciate it from a UIP pattern.
1.Asbestosis.
Pleural plaques,
round atelectasis,
subpleural plaques,
honeycombing often absent or less pronounced,
traction bronchiectasias not a predominant finding.
Fig. 7

Fig. 7: Axial and sagital chest CT images show calcified pleural plaques in the right anterior and posterior pleura (yellow arrows), pleuroparenchymal bands (blue arrows), and peripheral reticular pattern of lower lobe predominance (red arrows).
References: Department of Radiology, University Hospital Santa Lucía
2.
NSIP (non specific interstitial pneumoniae): ground glass opacities as the predominant findings,
peribroncovascular predominance,
honey combing less extent than UIP or absent.
Pleural effusion,
oesophageal dilation,
or pericardial abnormality also supports the diagnosis of NSIP due to collagenvascular disease. Fig. 8
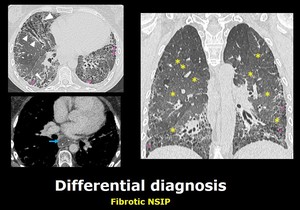
Fig. 8: Chest CT scan of a female patient with scleroderma. There is a diffuse increased in the density of the lung parenchima (yellow asterisk) in keeping with diffuse ground glass opacities. There are also traction bronchiectasis (arrowheads) as well as honeycombing (pink asterisk) of peripheral distribution. With mediastinal window, esophageal dilation, (which has a nasogastric tube inside) related to her collagenopathy can be depicted (blue arrow).
References: Department of Radiology, University Hospital Santa Lucía
3.Chronic hypersensitivity pneumonitis: Suspect it if there are poorly defined fine micronodules airtrapping,
or sparing of the lung bases.
Upper or mid-lobe predominance.
· Complications
-Pulmonary hypertension: Fibrosis of the lung parenchyma can leed to this complication. Fig. 9
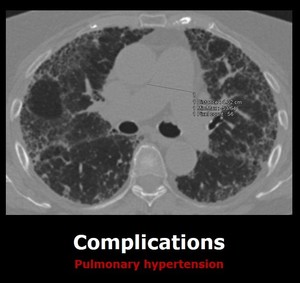
Fig. 9: Axial chest CT of a patient with IPF. There is enlargement of the main pulmonary artery in keeping with pulmonary hypertension.
References: Department of Radiology, University Hospital Santa Lucía
-Exacerbations: Exacerbations may be triggered by a clinical event (e.g.,
infection,
aspiration,
or drug toxicity) but are frequently idiopathic. Fig. 10
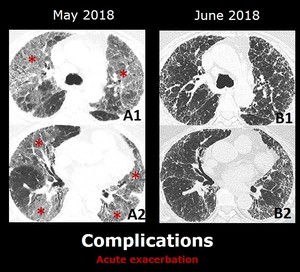
Fig. 10: Axial images from a patient with IPF .
A (1 and 2): there are ground glass opacities (*) in the upper lobes, middle lobe, lingula and lower lobes. There is also sparing of the anterior portion of the medial segment of the middle lobe and the anterior right lower lobe.
B(1 and 2): one month after treatment, there is complete resolution of the ground glass opacities.
References: Department of Radiology, University Hospital Santa Lucía
-Lung cancer: since these patients are heavy smokers,
there is an increase in the incidence of lung cancer (10-20%).



.
References: Department of Radiology, University Hospital Santa Lucía")
 and coronal (B) chest CT scans show reticulation (arrows), traction bronchiectasis (arrowheads) and honeycombing (*) with a heterogeneous distribution but basal and subpleural predominance. These findings are consistent with a typical UIP pattern.
References: Department of Radiology, University Hospital Santa Lucía")
 and traction bronchiectasis (arrowheads) with subpleural and basal predominance. There is also absence of honeycombing. All of these findings are consistent with a Probable UIP pattern.
References: Department of Radiology, University Hospital Santa Lucía")
 , traction bronchiolectasis (orange arrows), ground glass opacities (orange *) and air trapping (*). These findings are bilateral and asymmetrical and have an upper lobe predominance.
References: Department of Radiology, University Hospital Santa Lucía")
, pleuroparenchymal bands (blue arrows), and peripheral reticular pattern of lower lobe predominance (red arrows).
References: Department of Radiology, University Hospital Santa Lucía")
 in keeping with diffuse ground glass opacities. There are also traction bronchiectasis (arrowheads) as well as honeycombing (pink asterisk) of peripheral distribution. With mediastinal window, esophageal dilation, (which has a nasogastric tube inside) related to her collagenopathy can be depicted (blue arrow).
References: Department of Radiology, University Hospital Santa Lucía")

: there are ground glass opacities (*) in the upper lobes, middle lobe, lingula and lower lobes. There is also sparing of the anterior portion of the medial segment of the middle lobe and the anterior right lower lobe.
B(1 and 2): one month after treatment, there is complete resolution of the ground glass opacities.
References: Department of Radiology, University Hospital Santa Lucía")