ECR 2019 / C-0707
True or False: Gastrointestinal Diverticula and Complications
Congress:
ECR 2019
Poster Number:
C-0707
Type:
Educational Exhibit
Keywords:
Abdomen, Gastrointestinal tract, Anatomy, CT, MR, Fluoroscopy, Contrast agent-oral, Diverticula
Authors:
N. Kinger1, P. Mittal2; 1Atlanta, GA/US, 2Decatur, GA/US
DOI:
10.26044/ecr2019/C-0707

Fig. 1:
True versus False Diverticulum

Fig. 2:
Types of Diverticula

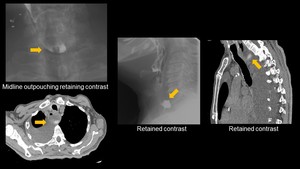
Fig. 3:
Zenker's Diverticulum

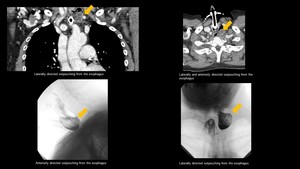
Fig. 4:
Killian-Jameson Diverticulum

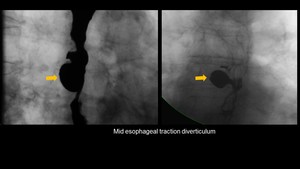
Fig. 5:
Traction Diverticulum

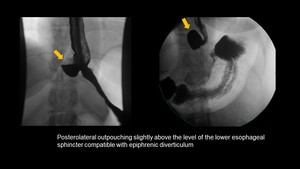
Fig. 6:
Epiphrenic Diverticulum

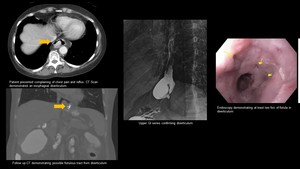
Fig. 7:
Esophageal Diverticulum with Esophageal Fistula

Fig. 8:
Esophageal Pseudodiverticulosis

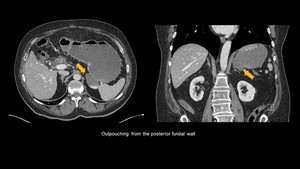
Fig. 9:
Gastric Diverticulum

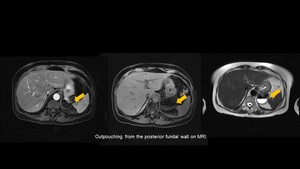
Fig. 10:
Gastric Diverticulum on MRI

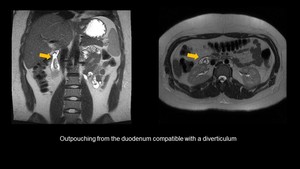
Fig. 11:
Duodenal Diverticulum

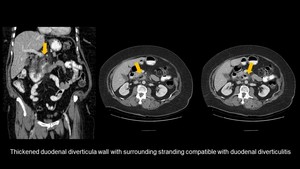
Fig. 12:
Duodenal Diverticulitis

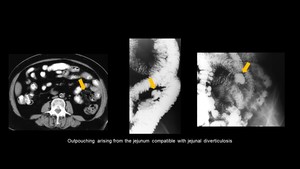
Fig. 13:
Jejunal Diverticulosis

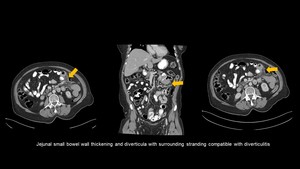
Fig. 14:
Jejunal Diverticulitis

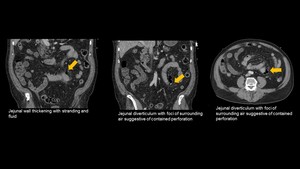
Fig. 15:
Jejunal Diverticulitis with Perforation

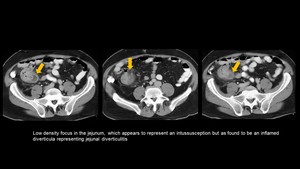
Fig. 16:
Jejunal Diverticulitis Mimicking Intussusception

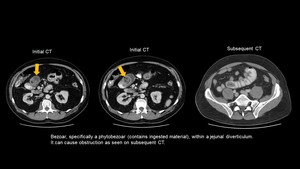
Fig. 17:
Jejunal Diverticulum with Bezoar

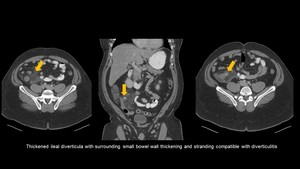
Fig. 18:
Ileal Diverticulitis

Fig. 19:
Meckel's Diveritculum

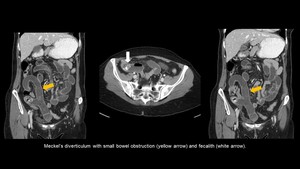
Fig. 20:
Meckel’s Diverticulum with Small Bowel Obstruction and Fecalith

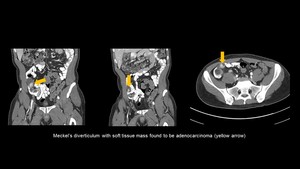
Fig. 21:
Meckel’s Diverticulum with Cancer

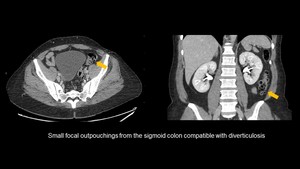
Fig. 22:
Colonic Diverticula

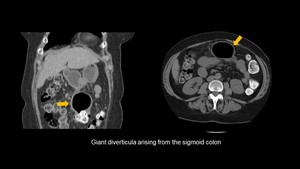
Fig. 23:
Giant Colonic Diverticulum

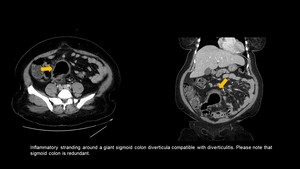
Fig. 24:
Giant Colonic Diverticulum with Diverticulitis

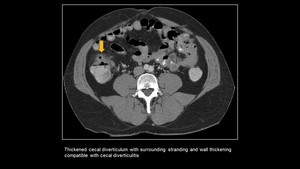
Fig. 25:
Cecal Diverticulitis

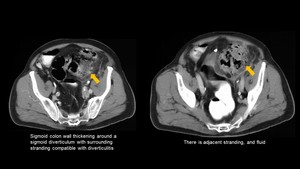
Fig. 26:
Diverticulitis of the Sigmoid Colon

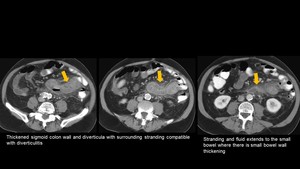
Fig. 27:
Colonic Diverticulitis with Reactive Small Bowel Inflammation

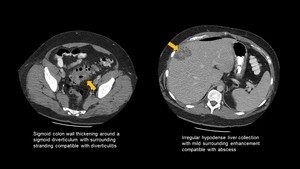
Fig. 28:
Colonic Diverticulitis with Liver Abscess

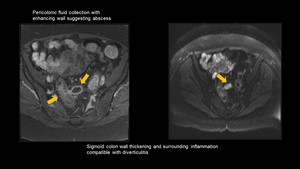
Fig. 29:
Colonic Diverticulitis with Abscess

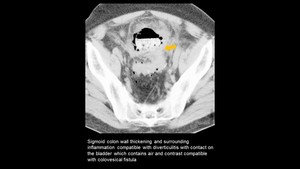
Fig. 30:
Colonic Diverticulitis with Colovesicular Fistula

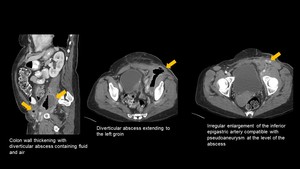
Fig. 31:
Diverticular Abscess with Inferior Epigastric Pseudoaneurysm

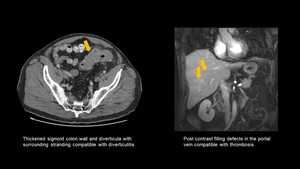
Fig. 32:
Colonic Diverticulitis with Portal Vein Clot