ECR 2019 / C-0734
A review of Urethrogram technique and imaging findings.
Congress:
ECR 2019
Poster Number:
C-0734
Type:
Educational Exhibit
Keywords:
Trauma, Cystography / Uretrography, Fluoroscopy, Urinary Tract / Bladder
Authors:
F. J. Azpeitia Armán1, R. M. Lorente Ramos1, J. M. LÓPEZ ARCAS CALLEJA1, M. Grande Barez2, A. Blazquez Saez3, P. Torres Rubio1; 1MADRID/ES, 228031 Madrid/ES, 3Salamanca/ES
DOI:
10.26044/ecr2019/C-0734

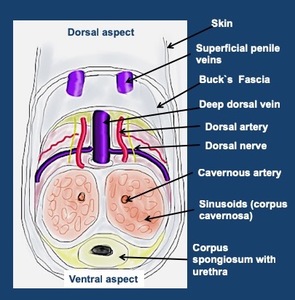
Fig. 1:
Urethra Anatomy

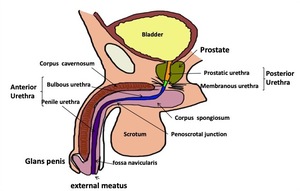
Fig. 2:
Urethra Anatomy
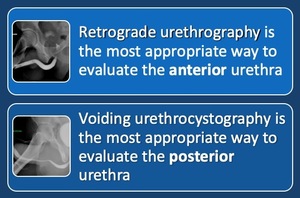
 and the bulbar urethra (blue arrow). The posterior urethra: membranous (red arrow) and prostatic urethra (green arrow) is best evaluated with voiding studies.")
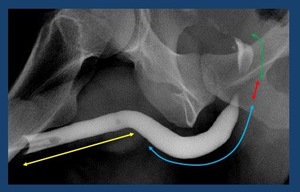
Fig. 3:
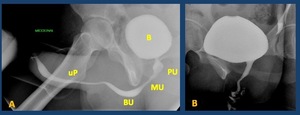
Normal retrograde urethrography. The anterior urethra, is formed by the penile...
 . MU: membranous urethra. The bulbar urethra (BU) and especially the penile urethra(uP) are better evaluated in retrograde studies in which a better repletion is achieved. B: bladder")
Fig. 4:
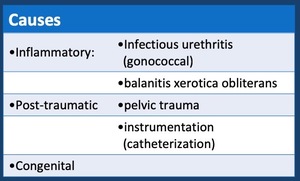
Normal voiding urethrography. It depicts the posterior urethra. PU. Prostatic...

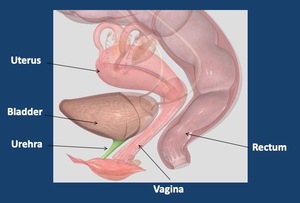
Fig. 5:
Female urethral anatomy

Fig. 6:
48 yo female: Voiding urethrogram

Fig. 7:
Retrograde urethrogram

Fig. 8:
Special tweezers for urethrography. A Tweezers with special end to pull the...
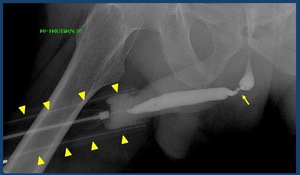
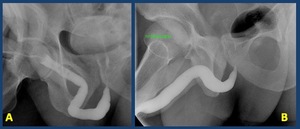
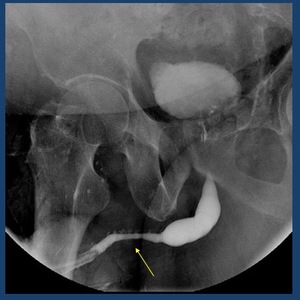
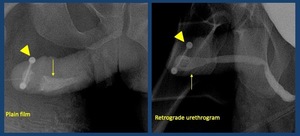
 showing a stenosis in the bulbar urethra (arrow).")
Fig. 9:
Retrograde urethrogram performed with forceps (arrowheads) showing a stenosis...

Fig. 10:
Preliminary film: AP and oblique view

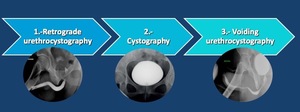
Fig. 11:
Study protocol

Fig. 12:
Retrograde and anterograde urethrography

B.-Retrograde urethrography performed through a perineal meatus")
Fig. 13:
A.- Retrograde urethrography: tip of the Foley’s catheter in the fossa...
 B.- Opacified Littre Glands (arrows)")
Fig. 14:
A.- Opacified Cowper duct (arrow) B.- Opacified Littre Glands (arrows)
 and vas deferens (arrowheads)")
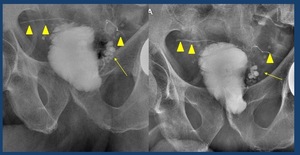
Fig. 15:
Contrast reflux to seminal vesicles (arrows) and vas deferens (arrowheads)
")
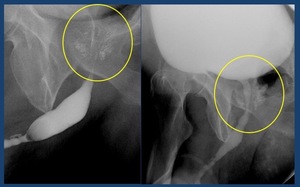
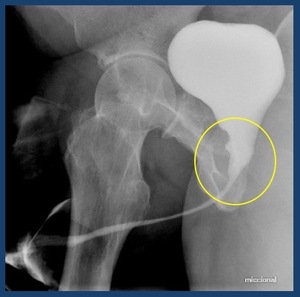
Fig. 16:
Contrast reflux to prostatic ducts (circle)
")
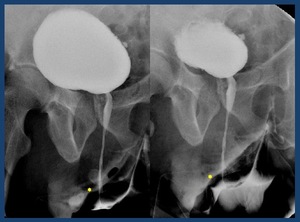
Fig. 17:
Retrograde urethrography: Contrast intravasation. Contrast fills the dorsal...
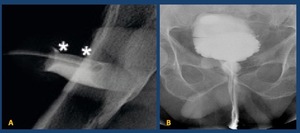
. B. When the pressure to fill the bladder is increased against the stenosis there is a contrast intravasation (asterisks)")
Fig. 18:
Retrograde urethrography: Contrast intravasation. A. Patient with stenosis in...
.")
Fig. 19:
Retrograde urethrography: bad technique. The probe has not been well purged and...

Fig. 20:
Incorrect patient positioning . Patient in oblique positioning and stretched...

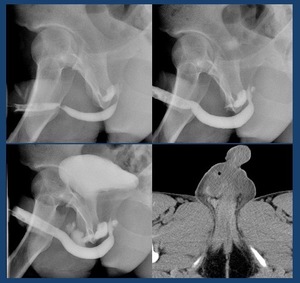
Fig. 21:
RUG and CT show extravasation of contrast material from the posterior urethra;...

Fig. 22:
Cystography
 . MU: membranous urethra. The bulbar urethra (BU) and especially the penile urethra (uP) are better evaluated in retrograde studies in which a better repletion is achieved.
B. Normal female voiding urethrography. .")
Fig. 23:
A. Normal male voiding urethrography. The Anterograde urethrography. PU....
")
Fig. 24:
Vesicoureteral reflux (arrows)

Table 1:
Causes of urethral stenoses

Fig. 25:
Retrograde urethrogram depicts a long irregular stricture of the penile urethra...

Fig. 26:
A.- Retrograde urethrogram: segment of irregular narrowing of the proximal...
")
Fig. 27:
Female Urethral stricture (arrow)

Fig. 28:
Gonococcal urethritis. stricture of the penile urethra
")
Fig. 29:
64 yo male. Urethral diverticulum (arrow)
")
Fig. 30:
63 yo female. Voiding cystourethrogram shows contrast filling urethral...
")
Fig. 31:
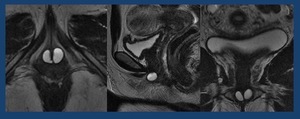
68 yo female. Multilocular Urethral diverticulum. Axial, sagittal and coronal...

Fig. 32:
Urethrorectal fistula in a patient undergoing prostatectomy

Fig. 33:
A and B.- Urethroperineal fistula. C.- Glans fistula. D.- Vesicovaginal fistula
. Piercing (arrowhead)")
Fig. 34:
Urethral Calculi in anterior urethra (arrow). Piercing (arrowhead)
")
Fig. 35:
Urethroplasty with oral mucosa of the bulbar urethra (arrow)
")
Fig. 36:
Radical prostatectomy: cavity post-prostatectomy (circle)
")
Fig. 37:
Perineal Urethroplasty. Perineal meatus (*)