Type:
Educational Exhibit
Keywords:
Fistula, Localisation, Diagnostic procedure, Complications, Fluoroscopy, CT, Conventional radiography, Lung, Genital / Reproductive system female, Gastrointestinal tract
Authors:
M. A. S. sabawi1, M. A. H. Shah1, Z. W. N. Noori 2, A. Al-Taie1; 1Doha/QA, 2Northyork/CA
DOI:
10.26044/ecr2019/C-1085
Findings and procedure details
Iatrogenic renal arteriovenous fistula (AVFs):
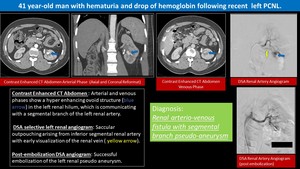
Fig. 1: Iatrogenic renal arteriovenous fistula
- Iatrogenic causes e.g.
kidney biopsy,
blunt or penetrating trauma,
inflammation,
etc.
constitute about 70 % of renal AVFs etiologies 1.
- Could be a cause of persistent hematuria,
uncontrolled hypertension and/or sudden or progressive decline in the renal function 2.
- Serious sequelae include high-output heart failure and distal thromboembolization are reported as well 2.
- Digital subtraction angiography is the gold standard for diagnosis of renal AVF; however,
it is invasive 1,3.
Non-invasive modalities include US and CT angiography.
- Ultrasound: Renal AVFs are usually not seen easily in B-mode.
Color Doppler images will show “visible thrill” or “soft tissue bruit”.
Spectral Doppler tracings show a high-velocity,
low resistance flow within the artery and turbulent,
pulsatile,
arterialized flow in the segmental draining vein.
- CT angiography will show the abnormal renal arteriovenous communication with associated aneurysms and early opacification of the renal vein on the arterial phase 3.
Iatrogenic tracheoesophageal fistula (TEF):
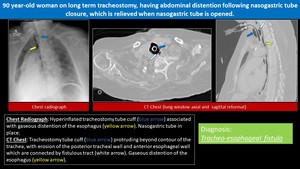
Fig. 2: Iatrogenic tracheoesophageal fistula
- Iatrogenic etiology represent a second most common cause of acquired TEF (malignancy represent is the most common cause) 4.
- TEF is a rare but serious complication of tracheostomy (incidence ≤ 1%) 5.
- The fistulous tract bypasses the normal protection provided by the physiological laryngeal reflexes,
causing repeated pulmonary aspiration.
- TEF should be suspected in any ventilated patient who has unexplained weight loss,
recurrent pulmonary aspiration and repeated failures to wean.
- In non-ventilated patient,
it should be considered in case of uncontrolled coughing after swallowing ‘Ono's sign’ 4.
- A chest X-ray will demonstrate the effects of repeated aspiration.
- Diddee et al suggested that an over-inflated cuff,
wider than the tracheal diameter,
may be a clue to a cuff-related TOF 4.
- A barium swallow demonstrates the defect in 70% of lesions 4.
- Endoscopy is the best diagnostic method.
- No large studies had been published to establish the diagnostic role of CT scan in the evaluation of adult TEF (in contrast to neonatal TEF) 6.
Iatrogenic Gastrobronchial Fistula:
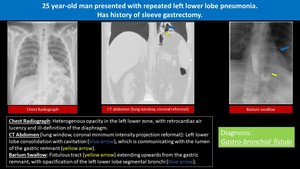
Fig. 3: Iatrogenic Gastrobronchial Fistula
- Iatrogenic causes include gastro-oesophageal surgery,
subphrenic abscess,
trauma,
gastric ulcer,
neoplastic and miscellaneous 7.
- Gastrobronchial fistula(BGF) is a rare but serious complication of laparoscopic sleeve gastrectomy with significant morbidity and mortality 9.
- Suggestive clinical presentation includes persistent cough,
sometimes associated with liquid or food ingestion,
hemoptysis,
wheezing,
pleuritic pain,
and findings consistent with left pleural effusion or lung consolidation.
Fever,
leukocytosis,
hypoxemia,
or frank sepsis may be present 11.
- A contrast study of the upper gastrointestinal tract is the most successful means of diagnosing Gastrobronchial fistula 7.
- CT scan is helpful in diagnosis,
it also shows mediastinal,
pulmonary and subphrenic abscesses,
recurrent pneumonia,
and an associated pleural effusion 12,13.
- The fistula may connect at any site in the respiratory tract so as to be difficult to locate,
and may not be visualized during bronchoscopy; in such cases,
a methylene blue dye test may show bluish sputum 12.
- Upper endoscopy does not diagnose GBF,
but can identify the internal opening,
can assess the anatomy of the stomach and can be used for therapeutic purposes,
thus minimizing the need for invasive surgery 10.
Iatrogenic Vesico-Uterine Fistula:
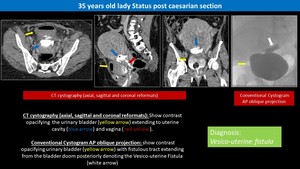
Fig. 4: Iatrogenic Vesico-Uterine Fistula
- It represents a rare urogenital complication,
accounting for approximately 1-4 % of genitourinary fistulas 14.
- VUF is considered to be the least common type of genitourinary fistulas 14.
- In general,
most common causes of urogenital fistulas are obstetric,
surgical,
or related to tumor,
or radiation necrosis 15.
- A main cause of VUF is an iatrogenic injury during Caesarean section,
particularly dissection of the lower uterine segment 15.
- Patients with vesicouterine fistula classically present with cyclic hematuria (menouria),
the absence of vaginal bleeding (amenorrhea),
and complete urinary continence 16.
- In rare occasions,
urinary incontinence could also be a clinical presentation in patients with vesicouterine fistula,
especially with the involvement of the cervix or the fistula is infra isthmic 16.
- Cystoscopy and vaginoscopy often show abnormalities.
However,
fistula sites may not be visualized 18.
- Cystography or VCUG may be required for diagnosis and characterization of the tract.
Excretory urography may be useful to exclude a concomitant ureterovaginal fistula,
which is associated with up to 10% of patients 18.
- Delayed contrast-enhanced CT has also been advocated.
Findings include excretion of intravenous contrast material into the vagina was observed in 60% of cases,
strongly suggesting the diagnosis.
Air or fluid in the vagina may also be present 18.
Iatrogenic Vesico-Vaginal Fistula:
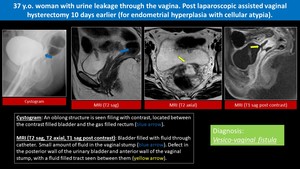
Fig. 5: Iatrogenic Vesico-Vaginal Fistula
- Vesicovaginal fistulas usually occur as a complication of childbirth in developing countries and as complications of gynecologic procedures in developed countries 18.
- Overall incidence of VVFs after hysterectomy during 2000– 2005 was 0.16% 19.
- Most common symptom in patients with VVF is constant urine drainage per vagina causing significant burden for a patient,
due to its numerous psycho-social consequences 17,20.
- Cystoscopy and vaginoscopy often show abnormalities.
However,
fistula sites may not be visualized 18.
- Cystography or VCUG may be required for diagnosis and characterization of the tract.
Excretory urography may be useful to exclude a concomitant ureterovaginal fistula,
which is associated in up to 10% of patients 18.
- Delayed contrast-enhanced CT has also been advocated.
Findings include excretion of intravenous contrast material into the vagina was observed in 60% of cases,
strongly suggesting the diagnosis.
Air or fluid in the vagina may also be present 18.
Iatrogenic Entero-Cutaneous Fistula:
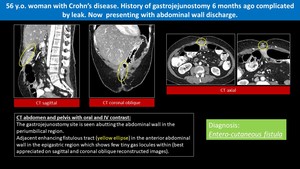
Fig. 6: Iatrogenic Entero-Cutaneous Fistula
- Nowadays,
the majority (~80%) of ECFs develops secondary to abdominal surgeries (iatrogenic); alternative,
less common causes include chronic inflammatory bowel diseases (IBD) such as Crohn’s disease,
tumors,
and radiation enteritis in descending order of frequency 21.
- Characterization is usually made on the basis of anatomy (site of origin,
simple or complex fistula,
end or lateral fistula,
presence or absence of distal obstruction) or fistula output (with high output usually defined as more than 500 ml per 24 hrs.) 22.
- Key features suggestive of an ECF include abdominal pain,
tenderness,
prolonged ileus,
signs of wound infection,
distention,
and enteric contents draining from an abdominal site.
Fever,
as well as tachycardia,
would be significant for localized or diffuse peritonitis 23.
- Radiographic studies helpful for delineation of the fistula include plain radiography,
gastrointestinal contrast studies,
fistulograms,
ultrasound,
and computed tomography scanning.
- Fistulography performed by the injection of water-soluble contrast into the fistulous tract,
is useful to determine the length of the tract,
the location of the fistula,
and the extent of bowel wall disruption.
- Computed tomography scanning has largely replaced fistulograms for fistula delineation and is able to demonstrate not only the anatomy and origin of the tract,
but also rule out intra-abdominal abscess cavities and interloop abscesses.
It also can rule out distal obstruction as well as delineate the presence of any foreign bodies 23.
Iatrogenic Aortogastric Fistula:
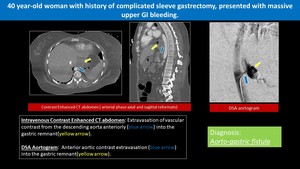
Fig. 7: Iatrogenic Aortogastric Fistula
- Aortogastric fistula (AGF) represent abnormal communications between the stomach and the aorta due to medical intervention.
- The aorto-gastric fistula is a very rare and fatal condition,
commonly result in rapid hemorrhage with a high mortality rate.
- Twenty-one cases of aortogastric fistula have been reported in the literature,
and only one patient survived after undergoing surgery and endovascular stent graft placement 24.
- Clinical presentation includes upper GI bleeding,
sepsis,
and abdominal pain,
but the condition also may be clinically occult.
- Because clinical signs may be occult or may not be sufficiently specific,
imaging is most often necessary to achieve an accurate diagnosis.
- CT scan of the abdomen with IV contrast is the imaging modality of choice for evaluations in the emergency setting,
owing to its widespread availability and high efficiency 25.
- Although conventional angiography is rarely used as the first-line imaging modality for the diagnosis of aortogastric fistula,
it may be helpful for surgical planning in certain cases 25.
- Angiography with embolization therapy or stent placement also may be used to treat massive gastrointestinal bleeding secondary to an aortogastric fistula 25.
Iatrogenic Pyelo-venous Fistula:
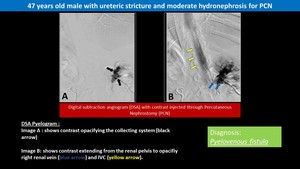
Fig. 8: Iatrogenic Pyelo-venous Fistula
- It always results from the synchronous rupture of a vein together with the fornix.
- Pyelo-venous fistulae are rare and represent the least common among urinary fistulas with their real incidence remains unknown 27,28.
- Antegrade or retrograde pyelography may show the Pyelo-venous fistula 29.








