Once learned that the presence of ectopic gas can be related to a wide spectrum of clinical situations,
in this section a etiopathogenic approach will be made.
1.
ECTOPIC GAS OF IATROGENIC ORIGIN
TENSION PNEUMOCEPHALUS
Also known as intracraneal aerocele, this entity is characterized by presence of air within the subdural space.
It is considered a neurosurgical emergency due to the mass efect the pneumocephalus provokes against the underlying cerebral parenchyma,
with subsequent permanent neurological damage.
Most of the times it is secondary to an unidirectional valvular mechanism of air entrance, which explains the necessity of decompression surgery.
The following causes are the most widely described as responsible for tension pneumocephalus:
- Traumatic
- Neurosurgery.
In particular,
surgical procedures involving posterior cerebral fossa and cervical region,
mostly when the patient is in sedestation.
Also when chronic subdural hematomas are surgically drained (incidence of 5% approx.).
- Less common causes: infections,
use of nitrous oxide as anesthesic agent,
etc.
On cross-sectional images,
tension pneumocephalus alters the morphology of frontal lobes,
giving the silhouette-like appearance of Mount Fuji,
once the cerebral convexity is lost.
Fig. 2
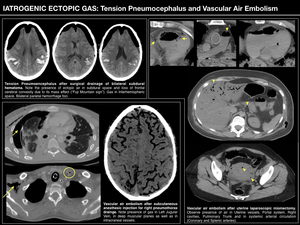
Fig. 2
VASCULAR AIR EMBOLISM
Vascular air embolism is a rare but potentially lethal condition,
where air bubbles burst into the intravascular space provoking vascular occlusion.
It is secondary to a pathologic communication between the vascular space (usually venous) and a certain air reservoir.
A pressure gradient (such as bipedestation,
anti-Trendelenburg,
deep inspiration,
hypotension or hypovolemia) that favours gas spread is also necessary to produce a clinically significant vascular air embolism. Fig. 2 Fig. 3

Fig. 3
RETAINED SURGICAL FOREIGN BODY / GASOMA
Gasoma or gossypiboma makes reference to a retained foreign body (usually surgical) and the correspondant tisular reaction it provokes.
Thus,
it is a exogenous-endogenous mass which could be harmful owing to the following two reactions:
- Fibrinous asepctic reaction.
A foreign-body reaction occurs,
resulting in adherence formation.
Patients can present with intestinal obstructive symptoms and chronic inflammatory pain.
- Exudative reaction.
When a superinfection happens,
the retained foreign body might lead to an abscess formation.
Fig. 4
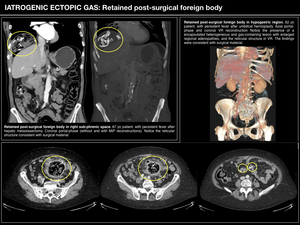
Fig. 4
2.
NEOPLASTIC ECTOPIC GAS
Ectopic gas related to malignant diseases is a condition to bear in mind,
as most of the tumours causing it are malignant,
which might have a deleterious effect on the patient's prognosis.
Although most of the neoplasms causing ectopic gas are GI tract tumours,
with almost 10% of colorectal carcinomas presenting with perforation with secondary pneumoperitoneum,
other tumours,
such as lung cancer can also cause fistulizations between different anatomical structures provoking ectopic gas.
Fig. 5
Although identification of the perforation or fistulae by CT is important,
diagnosis of the underlying cause will be more critical in terms of administering proper management,
as the majority of these cases will require surgical solutions.
3.
ECTOPIC GAS OF SPONTANEOUS ORIGIN
INTERSTITIAL PNEUMOMEDIASTINUM
Pneumomediastinum is defined as presence of air within mediastinum.
Its main causes are:
- Surface-barrier damage (tracheo-bronchial tree or esophageal rupture).
- Alveolar rupture,
which causes interstitial pneumomediastinum or Macklin effect. It constitutes the most important cause of pneumomediastinum,
both in traumatic and spontaneous contexts.
In fact,
severe traumatic pneumomediastinum is caused by Macklin effect in almost half of the cases. Fig. 5
GAS WITHIN GALLSTONES
This radiological finding is a "benign" cause of ectopic gas and is also known as "Mercedes-Benz sign",
after the triradiate pattern the gas within gallastones acquires.
It is secondary to fissures created on the surface of gallstones during the cristalization process,
in particular in "soft" gallstones,
such as cholesterol-cholelythiasis.
It is interesting to be familiarized with this finding in order not to get confused with real pathological findings. Fig. 5
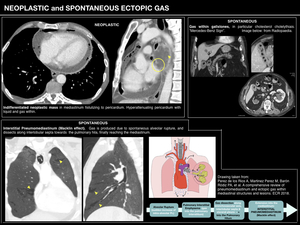
Fig. 5
4.
TRAUMA-RELATED ECTOPIC GAS
TENSION-PNEUMOTHORAX
Whenever a pneumothorax is diagnosed in the Emergency Department,
tension pneumothorax should be ruled out,
which is diagnosed relying on the following radiological features (Fig. 6):
- Contralateral mediastinal displacement.
- Intercostal spaces are increased due to hyperinsuflation.
- Diaphragmatic dome is flattened,
or even inverted.
Radiological diagnosis of the most frightnening complication of the tension pneumothorax,
the cardiogenic shock,
is based on the next features:
- Contrast reflux to Inferior Vena Cava and Hepatic Veins,
which traduces Right Ventricular Failure.
- Gathering of contrast in declive zones,
observing blood-contrast levels owing to reduced venous return.
- Absence of contrast in left cavities indicates cardiorrespiratory arrest: the CT study must be stopped to initiate the cardiopulmonary resuscitation maneuvers.
However,
patients should be first estabilized and with airway and breathing under control before the CT is performed,
as the ATLS (Advanced Trauma Life Support ) guidelines state.
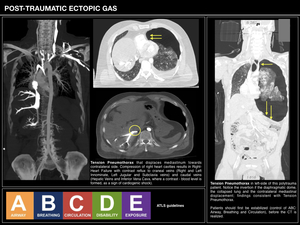
Fig. 6
5.
INFECTIOUS-INFLAMMATORY ECTOPIC GAS
EMPHYSEMATOUS INFECTIONS
Emphysematous infections are caused by gas-forming bacteria (anaerobic and gram-negative bacteria,
specially enterobacteria).
These infections represent potentially life-threatening conditions that require aggressive medical and often surgical management.
Because rapid progression to sepsis usually occur in the absence of early therapeutic intervention,
early diagnosis including imaging techniques is essential.
Although emphysematous infections could be suspected by US or radiographs,
CT should always be used for confirmation and precise extension and localization.
These infections include emphysematous cholecystitis,
pancreatitis,
cystitis,
pyelonephritis,
gastritis,
gas gangrene of the uterus and Fournier's gangrene.
The first three entities are represented in Fig. 7 and a special mention to necrotizing fasciitis and Fournier's gangrene is made in Fig. 8.
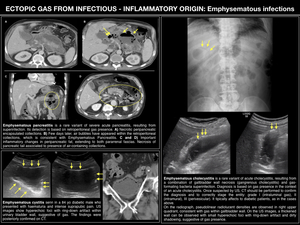
Fig. 7
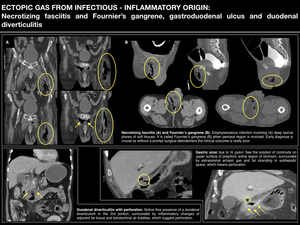
Fig. 8
GASTRODUODENAL ULCUS
After H.pylori was discovered to be the causal agent of gastroduodenal ulcus and once effective antibiotherapies established,
its incidence has decreased significantly in Europe.
However,
it is important to know its main potential complications: digestive haemorrhage and perforation,
as surgical management is usually requiered due to high morbimortality rates. Fig. 8
DIVERTICULITIS
Diverticulitis is one of the symptomatic presenting features of diverticular disease,
along with lower gastrointestinal haemorrhage ("diverticular haemorrhage").
Gastrointestinal and colonic diverticula are almost all false diverticula: mucosa herniations thruogh a defect in the muscularis,
covered by overlying serosa.
Sigmoid colon and descending colon are the most usual localizations,
followed by duodenum. Fig. 8
Although most of the times,
diverticulitis has no major complications,
radiologists should be familiarized with the potential complications of diverticulitis,
which include abscess formation,
fistulization to adjacent structures,
perforation and post-inflammatory adherence formation.
INFECTIOUS AORTITIS
The vast majority of aortitis are non-infectious (secondary to rheumatological,
autoimmune disesases or paraneoplastic syndromes).
Nevertheless,
it is of sum importance to diagnose infectious aortitis due to its strong relationship to malignant diseases (in particular,
colorectal carcinoma and haematological malignancies).
Fig. 9
AORTO-ENTERIC FISTULAE
Aorto-enteric fistula is defined as an abnormal connection between the aorta and the gastrointestinal tract.
Aorto-duodenal fistulae are the most common type (∼60%) owing to the close relationship of the duodenum (in particular 3rd and 4th portions, which are tethered to the retroperitoneum),
with the underlying abdominal aorta.
They are most often the result of compression of an abdominal aortic aneurysm (AAA) or erosion of an aortic prosthetic graft into the surrounding gastrointestinal structures.
Secondary fistulae are far more common,
occuring as a consequence of surgery for an AAA,
usually after a prosthesis implantation.
Infection of an abdominal aortic prosthesis with enteroprosthetic fistula is a life-threatening complication that needs to be diagnosed as early as possible.
It should be always suspected in patients with an abdominal aortic prosthesis who present even the slightest rectorrhagia or melaena,
abdominal pain or sepsis.
It also could be revealed by clinical signs of hypertrophic osteopathy.
CT criteria providing evidence of a fistula are:
- Presence of gaseous images in a periprosthetic fluid collection.
- Thickening and/or retraction of the intestinal walls in contact.
- Existence of a false aneurysm.
- Extravasation of contrast into the intestinal lumen. Fig. 9
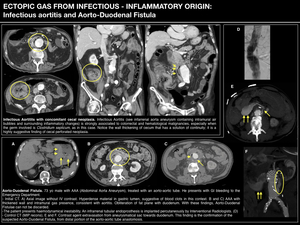
Fig. 9
6.
PNEUMATOSIS INTESTINALIS
Pneumatosis intestinalis makes reference to the presence of intramural gas of the GI tract.
It is a radiological sign and should not be considered as a certain diagnosis with a correspondant treatment,
owing to its multifactorial character.
Pneumatosis intestinalis could be present in a variety of different situations,
both "benign" and malignant or life-threatening.
|
BENIGN causes
|
LIFE -THREATENING causes |
- Systemic or Autoimmune disease: Lupus,
Polymyositis,
Sjögren Sd,
sarcoidosis.,
etc.
- Infectious: HIV / AIDS,
Varicella-Zoster V.,
Cytomegalovirus,
TBC,
etc.
- Organ transplantation: hepatic,
renal,
blood stem cell.
- Drugs: Corticoid,
Chemotherapy.
- Pulmonary disease: Pulmonary Obstructive Chronic Disease,
emphysema,
lung fibrosis,
etc.
- Gastrointestinal: pyloric stenoses,
bowel obstruction,
adynamic ileus,
Chron & Ulcerous Colitis,
diverticulitis,
Whipple,
carcinoma,
etc.
- Iatrogenia: endoscopy,
surgery.
- Primary: idiopathic,
Cystoid Neumatosis Intestinalis.
|
- Bowel Ischemia
- Closed-Loop Obstruction
- Necrotizing Enterocolitis
- Toxic Megacolon
|
Pathogenesis of pneumatosis intestinalis is complex,
with two widely accepted hypotheses for its development (see Fig. 10).
Imaging considerations of pneumatosis intestinalis
The first step is intramural gas detection,
for which pseudopneumatosis has to be excluded,
as it is an important pitfall that may lead to misdiagnosis.
Pseudopneumatosis refers to the condition when intraluminal beads of gas are trapped within or between feces and the adjacent mucosal folds.
Such condition is more commonly seen in the cecum and ascending colon,
where and admixture of liquid stool and gas facilitates its occurrence.
An important sign that suggests pseudopneumatosis is the presence of a gas collection against the bowel wall that suddenly stops at the free gas-fluid level within the lumen; continuation of the gas along the bowel wall beyond the gas-fluid level,
on the other hand,
mostly suggests a true pneumatosis intestinalis.
Alarm signs related to clinical severity have to be detected next (extensive pneumatosis,
presence of ascites,
mesenteric vessels occlusion).
Bowel ischemia must be excluded first and foremost,
based on its imaging features( Fig. 10 ):
- Frequent but less specific findings: bowel wall thickening,
bowel dilation,
free peritoneal fluid,
mesenteric fat stranding and pneumoperitoneum.
- Specific findings for bowel ischemia: presence of portomesenteric venous gas,
decreased or absent wall enhancement,
solid organ infarctions or perfusion defects and arterial or venous mesenteric occlusion.
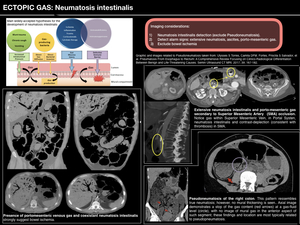
Fig. 10










