Radiographic Findings
Chest radiography is usually the first imaging method,
with 60-70% of patients having pathologic findings.
More than five decades ago,
Siltzbach developed a radiographic system that encompasses 5 stages,
according to the pattern of the findings Fig. 1 .
It defines the following five stages of sarcoidosis: stage 0,
with a normal appearance; stage I with bilateral hilar lymphadenopathy; stage II with hilar lymphadenopathy with pulmonary infiltrates; stage III with parenchymal infiltrates; and stage IV with irreversible fibrosis with parenchymal distortion or bullae.
The most common presentation at diagnosis is in the form of bilateral lymphadenopathy.
This classification system also has prognostic value,
with spontaneous remissions in 60%–90% of patients with stage I disease,
in 40%–70% with stage II disease,
in 10%–20% with stage III disease,
and in 0% with stage IV disease.
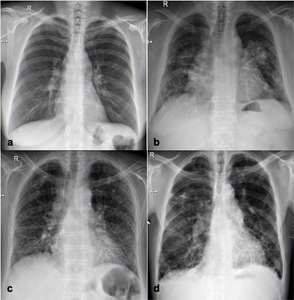
Fig. 1: Stages of sarcoidosis on the basis of chest radiographs. (a) Stage I with bilateral hilar lymphadenopathy. (b) Stage II with hilar lymphadenopathy with pulmonary infiltrates. (c) Stage III with parenchymal infiltrates. (d) Stage IV with parenchymal distortion due to fibrosis.
High-Resolution Computed Tomography
High-resolution CT (HRCT) allows better characterization of disease's extent and parenchymal findings,
improving detection of nodular and reticular opacities,
thickened interlobular septa,
and faint ground-glass opacities.
Furthermore,
HRCT allows differentiation of active inflammation from an irreversible disease.
Nodules,
ground-glass opacities,
alveolar opacities,
interlobular septal thickening,
and intralobular linear opacities are suggestive of granulomatous inflammation and are usually reversed with therapy.
On the contrary,
honeycomb-like cysts,
bullae,
architectural distortion,
volume loss,
and traction bronchiectasis are indicative of chronicity and fibrosis.
|
Inflammation,
reversibility
|
Chronicity and fibrosis
|
|
· Nodules;
· Ground-glass opacities;
· Alveolar opacities;
· Interlobular septal thickening;
· Intralobular linear opacities.
|
· Honeycomb-like cysts;
· Bullae;
· Architectural distortion;
· Volume loss;
· Traction bronchiectasis.
|
Mediastinal and hilar lymphadenopathy
Lymphadenopathy is the most common intrathoracic manifestation of sarcoidosis,
85% of cases),
usually in the form of symmetric bilateral hilar adenopathy with some form of paratracheal adenopathy Fig. 2 .
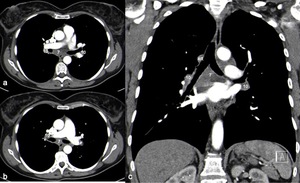
Fig. 2: Axial (a, b) and coronal (c) contrast material-enhanced CT scan (mediastinal window) showing bilateral and symmetric hilar (10), right paratracheal (4R) and infra-carinal (7) lymphadenopathy.
Mediastinal adenopathy without hilar involvement is rare and is more frequently seen in older patients.
Uncommon locations include isolated paratracheal adenopathy,
isolated aortopulmonary adenopathy,
isolated anterior mediastinal nodes,
isolated subcarinal lymphadenopathy,
and posterior mediastinal adenopathy.
These atypical patterns of lymphadenopathy occur more frequently in patients older than 50 years.
Hilar lymph node enlargement may be a feature of infection (particularly fungal or mycobacterial infection) or malignancy (lymphoma).
However,
symmetrical involvement in these pathologies is unusual.
Mediastinal and hilar lymph nodes may calcify in chronic sarcoidosis.
Amorphous calcifications are the most typical because they are not associated with other forms of granulomatous disease Fig. 3 .
Dense calcification is also commonly seen.
Egg-shell calcification,
as seen in silicosis,
is rare but has been observed.
Necrotic or low-density lymph nodes are rarely seen.
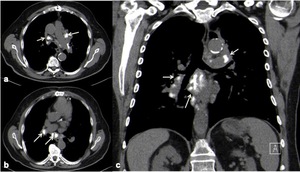
Fig. 3: Axial (a, b) and coronal (c) CT scan (mediastinal window) showing amorphous calcifications of hilar and mediastinal lymph nodes (arrows).
Typical Parenchymal findings
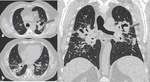
The most common parenchymal finding is the presence of small nodules with perilymphatic distribution in the subpleural peribronchovascular interstitium (75%–90% of cases).
High-resolution CT shows sharply defined,
rounded nodules,
measuring 1-5 mm,
usually with a bilateral and symmetric distribution,
mostly in the upper and middle zones (Fig. 4 and Fig. 5 ).
Due to the nodular involvement of the lymphatic system,
there is usually nodular or irregular thickening of the peribronchovascular interstitium.
The micronodules may coalesce over time,
forming larger lesions (macronodules).
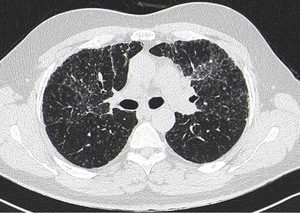
Fig. 4: Axial CT scan (lung window) shows the typical perilymphatic distribution of micronodules, with symmetric distribution.
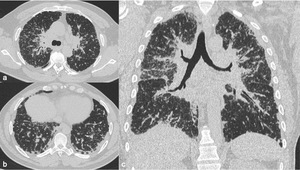
Fig. 5: Axial (a, b) and coronal (c) CT scan (lung window) show numerous small micronodules in perilymphatic distribution, with bilateral and symmetric involvement.
Atypical Parenchymal Findings
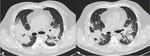
In 15%–25% of patients there are multifocal parenchymal opacities of varying sizes,
from 1 to 10 cm.
They tend to be multiple and bilateral,
most commonly in perihilar or peripheral location and radiate from the hilum toward the periphery and spare costophrenic angle ( Fig. 6 and Fig. 7 ).
The occurrence of cavitation of parenchymal lesions is rare,
being present in an estimated 10% of patients with end-stage disease ( Fig. 8 ).
Small satellite nodules are often visible at the periphery of these masses,
producing the "galaxy sign",
which may also be seen in the presence of other granulomatous diseases and neoplasms ( Fig. 7 ).
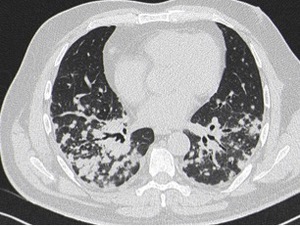
Fig. 6: Axial CT scan (lung window) shows numerous small nodules in perilymphatic distribution, with bilateral and symmetric involvement, radiating from the hilum toward the periphery.
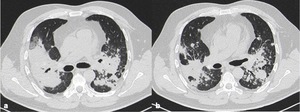
Fig. 7: Axial CT scans (lung window). There are areas of con�solidation resulting from the confluence of multiple parenchymal micronodules. Small satellite nodules are seen around the large nodules, producing the "galaxy sign".
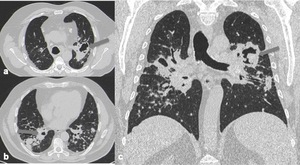
Fig. 8: Axial (a,b) and coronal (c) CT scans (lung window). There are bilateral areas of con�solidation, some of them with cavitation (arrows)
Patchy ground-glass opacities with ill-defined margins are seen in 40% of patients with parenchymal changes.
They are always accompanied by other abnormalities and often are superimposed on a background of interstitial nodules.
( Fig. 9 )

Fig. 9: Axial CT scan (lung window) shows multiple ground-glass opacities with ill-defined margins (arrows).
Isolated linear reticular opacities are observed in an estimated 50% of patients with sarcoidosis,
due to interlobular and intralobular septal thickening.
It is usually seen in the subpleural space in the upper and middle lung zones.
When it is marked and irregular it may simulate lymphangitic carcinomatosis.
However,
lymphangitic carcinomatosis is characterized by more extensive and more severe involvement of the interlobular septa and subpleural space.
In most patients,
sarcoid granulomas resolve with time.
However,
in 20-25% of patients,
fibrosis becomes more prominent over time,
with a typical distribution of upper and middle zone predominance.
Possible findings include linear opacities,
traction bronchiectasis,
and architectural distortion,
with a displacement of fissures and bronchovascular bundles.
Honeycombing is less common compared to other interstitial lung diseases,
and if seen,
tends to distribute subpleurally in the mid-upper zone,
sparing bases ( Fig. 10 ).
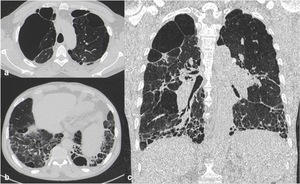
Fig. 10: Axial (a, b) and coronal (c) CT scan (lung window) show an atypical pattern of fibrosis, involving lower lung zones, as well as apical traction bronchiectasis and architectural distortion.
Pleural involvement in sarcoidosis is rare,
occurring in only 1%–4% of patients.
Pleural effusion is usually minimal and resolves within 2–3 months ( Fig. 11 ).
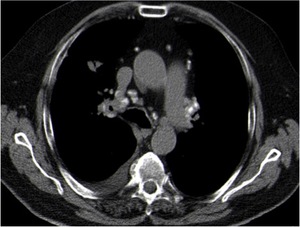
Fig. 11: Axial CT scan (mediastinal window) shows mediastinal lymph nodes with amorphous calcifications and right pleural effusion.

 Stage I with bilateral hilar lymphadenopathy. (b) Stage II with hilar lymphadenopathy with pulmonary infiltrates. (c) Stage III with parenchymal infiltrates. (d) Stage IV with parenchymal distortion due to fibrosis.")
 and coronal (c) contrast material-enhanced CT scan (mediastinal window) showing bilateral and symmetric hilar (10), right paratracheal (4R) and infra-carinal (7) lymphadenopathy.")
 and coronal (c) CT scan (mediastinal window) showing amorphous calcifications of hilar and mediastinal lymph nodes (arrows).")
 shows the typical perilymphatic distribution of micronodules, with symmetric distribution.")
 and coronal (c) CT scan (lung window) show numerous small micronodules in perilymphatic distribution, with bilateral and symmetric involvement.")
 shows numerous small nodules in perilymphatic distribution, with bilateral and symmetric involvement, radiating from the hilum toward the periphery.")
 shows multiple ground-glass opacities with ill-defined margins (arrows).")
 and coronal (c) CT scan (lung window) show an atypical pattern of fibrosis, involving lower lung zones, as well as apical traction bronchiectasis and architectural distortion.")
 shows mediastinal lymph nodes with amorphous calcifications and right pleural effusion.")