HYPOPHARYNGEAL/ESOPHAGEAL DIVERTICULUM
Fluoroscopic esophagram is the gold standard for diagnosis of diverticulum of the upper GI tract.
These diverticula are often incidentally discovered on fluoroscopic swallow studies performed for other indications.
A pitfall of this technique occurs when small diverticula are obscured by superposition on the main column of barium in the esophagus.
This can be overcome by rotating the patient. Using continuous video fluoroscopy in anteroposterior (AP) and lateral projections can improve sensitivity for small diverticula and show evidence of overflow or aspiration.

Fig. 3: (A) Lateral view barium esophagram demonstrates a Zenker’s diverticulum, which typically presents posteriorly with its sac above the cricopharyngeal bar. (B) AP view barium esophagram showing a Killian-Jamieson diverticulum which occurs inferior to the cricopharyngeus and lateral to the longitudinal esophageal muscle fibers. (C) AP view barium esophagram showing a midthoracic diverticulum. (D) AP view barium esophagram of an epiphrenic diverticulum just superior to the diaphragmatic crus(blue arrow).
-Zenker’s Diverticulum
- A false hypopharyngeal pulsion diverticulum that occurs in the Killian triangle,
between the fibers of the cricopharyngeus and the inferior constrictor. Fig. 4
- Most common diverticulum in the upper GI tract,
with a prevalence between 0.01 and 0.11%.
- Pathophysiology is related to high intraluminal pressures relative to the retropharyngeal space
- Commonly presents with dysphagia,
cervical borborygmus in the presence of a palpable neck lump,
hoarseness/dysphonia,
cough,
regurgitation,
malnutrition,
and halitosis.
- Complications include ulceration,
squamous cell carcinoma,
aspiration pneumonia,
and perforation during endoscopic procedures or nasogastric tube placement.
- Treatment is indicated for symptomatic cases with endoscopic or surgical techniques.

Fig. 5: Anteroposterior (A) and lateral (B) views of a Zenker’s Diverticulum after treatment with per oral endoscopic myotomy (Z-POEM).
-Killian-Jamieson Diverticulum
- False diverticulum anatomically distinct in that it occurs inferior to the cricopharyngeus and lateral to the longitudinal esophageal muscle fibers in an area known as Killian-Jamieson space. Fig. 6
- Incidence is approximately one fourth that of Zenker's
- Surgical management with excision of the diverticulum and esophageal myotomy is indicated for large and symptomatic cases.
- Endoscopic procedures are generally avoided given the proximity of the recurrent laryngeal nerve.
-Midthoracic Diverticulum
- Usually small and have a wide mouth. Fig. 7
- Often asymptomatic and found incidentally.
- Esophageal dysmotility and pulsion forces cause the majority of cases.
- Underlying motility disorders cause most of the symptoms and complications including retrosternal pain,
dysphagia,
regurgitation,
epigastric pain,
and recurrent pulmonary infections.
- Surgical correction is usually not required but can be done via thoracoscopy or thoracotomy.
-Epiphrenic Diverticulum
- False pulsion diverticula which occur in the distal 10 cm of the esophagus,
usually projecting from the right posterior wall. Fig. 8
- Less than 10% of esophageal diverticula,
affecting approximately 1:500,000.
- The majority of cases occur with a primary esophageal motility disorder such as achalasia or diffuse esophageal spasm,
where contractile discoordination between the distal esophagus and lower esophageal sphincter (LES) leads to increased intraluminal pressure.

Fig. 9: Fluoroscopic images showing esophageal dismotility with delayed emptying, reversed peristalsis, and an epiphrenic diverticulum (white arrow on the last image).
- Usually asymptomatic, but can present with dysphagia,
chest pain,
weight loss,
and regurgitation.
- Complications include nocturnal aspiration,
aspiration pneumonia,
perforation,
and rarely progression to carcinoma.
- In symptomatic patients,
intervention with diverticulectomy is accompanied by cardiomyotomy to correct the underlying motility disorder,
as well as partial fundoplication to prevent postoperative reflux.
- Non-surgical candidates may benefit from injection of botulinum toxin into the LES and esophagus distal to the diverticulum.
GASTRIC DIVERTICULUM
- Rare,
with prevalence ranging from 0.01%-2.6%.
- Usually less than 4 cm in size.
- More commonly congenital than acquired.
- Most congenital cases are located in the posterior wall of the gastric fundus,
approximately 2 cm below the esophagogastric junction and 3 cm from the lesser curve of the stomach. Fig. 10
- Acquired cases are usually located in the gastric antrum,
often secondary to peptic ulcer disease,
malignancy,
pancreatitis,
gastric outlet obstruction,
or after surgical procedures of the stomach.
- Usually asymptomatic and discovered incidentally,
but can present with a full,
painful,
or uncomfortable sensation in the upper abdomen,
dyspepsia,
nausea,
and emesis or with complications such as bleeding,
diverticulitis,
or rarely adenocarcinoma.
- Detection is usually accomplished by fluoroscopy or esophagogastroduodenoscopy.
- A known pitfall of CT is mistaking a gastric diverticulum for a retroperitoneal mass depending on location and intraluminal contents. (Fig. 11 below)
- Medical management with proton pump inhibitors can alleviate symptoms,
but is less effective for diverticula greater than 4 cm.
- Laparoscopic surgical resection is indicated for symptomatic patients with large diverticula.

Fig. 11: CT axial image of a gastric diverticulum (white arrowhead), which can be mistaken for an adrenal adenoma or other retroperitoneal mass depending on the location and intraluminal contents.
SMALL BOWEL DIVERTICULUM
Diverticula of the small bowel generally occur where the mesenteric vessels penetrate into the muscular layer,
presumably because of abnormalities in intestinal peristalsis,
intestinal dyskinesia,
and high intraluminal pressure. Most occur after age 40 and are asymptomatic. When symptoms do occur,
they can include abdominal cramping,
diarrhea,
and those related to complications such as diverticulitis,
abscess,
malabsorption,
volvulus,
bacterial overgrowth,
obstruction,
perforation,
hemorrhage,
as well as pancreatic and biliary disease in the case of the duodenum.
-Duodenal Diverticulum
- Second most common location of GI diverticula with a prevalence of 5-22%.
- Can be single or multiple and true,
false,
or intraluminal.
- True diverticula are less common than false diverticulum,
resulting from failed duodenal recanalization in utero and generally located in the medial aspect of the second and third portions of the duodenum.
- False diverticula are acquired and can have pulsion or less commonly traction etiologies,
such as duodenal ulcers or cholecystitis,
and most often occur at the ampulla.
- Intraluminal DD are pathologically duodenal mucosal webs and occur in the second or third portion of the duodenum and are associated with Down syndrome,
choledochocele,
and annular pancreas.
- Saccular outpouching appearance on barium fluoroscopy. Fig. 12
- On CT or MRI,
they often appear as a thin-walled,
rounded collection of gas or debris with gas fluid levels. Fig. 13 , Fig. 14
- Should be reported given the technical challenges they can pose should the patient need an endoscopic procedure in the future.
- May be difficult to distinguish from solid or cystic neoplasms of the pancreatic head,
and MRCP may aid in clarification.
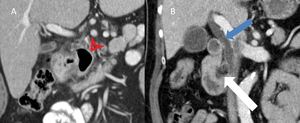
Fig. 15: (A) CT coronal image showing a gas-filled duodenal diverticulum (red arrowhead) with surrounding fat stranding consistent with duodenal diverticulitis. (B) CT coronal image showing a dilated common bile duct (blue arrow) secondary to duodenal diverticulum (white arrow) with intraluminal debris.
-Jejunoileal Diverticulum
- Usually acquired,
false pulsion diverticula and are approximately five times less common than DD.
- Pathogenesis is related to increased intraluminal pressure and subsequent weakening of the bowel wall with herniation of mucosa and submucosa through the muscular layer.
- Can be caused by abdominal surgery or conditions such as Crohn’s disease or tuberculosis.
- The majority of cases occur in the jejunum Fig. 16 .
Less commonly,
they can occur in the ileum or even less frequently both the jejunum and ileum.
- Mostly asymptomatic,
but can present with chronic non-specific symptoms such as abdominal pain,
constipation,
diarrhea,
or malnutrition.
- The mainstay of diagnosis is CT,
preferably with IV and oral contrast,
though it may underestimate disease burden.
- Enteroclysis by fluoroscopy,
CT,
or MRI offers better accuracy,
but rarely changes management.
- In diverticulitis,
fluid in the mesentery or peritoneal cavity seen on CT or MRI indicates severe disease though this can occasionally be difficult to distinguish from simple peritoneal fat stranding.
- Conservative management of diverticulitis involves antibiotics and bowel rest,
while surgical management includes resection of the involved small bowel.
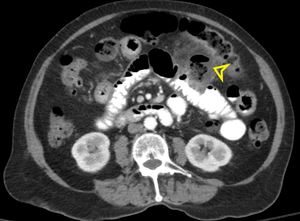
Fig. 17: CT axial view with oral contrast with a large outpouching (yellow arrowhead) in an opacified loop of jejunum (normal appearance of the jejunal folds) with surrounding inflammatory changes consistent with jejunal diverticulitis.
-Meckel’s Diverticulum
- The most common congenital diverticula of the GI tract
- Result from a persistent vitellointestinal duct
- Occur in about 2% of the population,
are often about 2 inches in length,
usually are located within 2 feet of the ileocaecal valve and often presents before age 2 (Rule of 2s).
- Complications associated with MD include bleeding,
obstruction,
diverticulitis,
and intussusception.
- Can be diagnosed on CT,
MRI,
or a nuclear medicine “Meckel’s scan.” Fig. 18 below
- Approximately 50% of Meckel’s diverticula contain ectopic gastric mucosa,
resulting in ectopic radiopharmaceutical uptake of technetium-99 pertechnetate in the mid abdomen.
- Surgical resection via a laparoscopic approach is indicated.
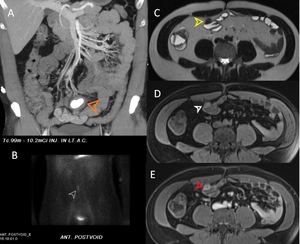
Fig. 18: (A) CT coronal maximum intensity projection image shows a Meckel’s diverticulum (MD) containing retained oral contrast material. (B) A nuclear medicine Meckel’s scan showing uptake in a MD lined with gastric mucosa. (C) T2-weighted MR image showing a small hypointensity off the distal ileum. (D) This area is hyperintense on T1-weighted images with fat saturation. (E) Enhancement on postcontrast T1-weighted imaging is consistent with an MD.
APPENDICEAL DIVERTICULUM
- Can be congenital or acquired.
- Acquired AD are most commonly seen in the distal third of the appendix at the mesenteric edge (Fig. 19 below) and may be seen more commonly in males as well as people affected with Hirschsprung's disease or cystic fibrosis.
- Congenital AD are more commonly seen on the antimesenteric edge and are associated with Patau syndrome (trisomy 13).
- Appendiceal diverticulitis often presents with more mild clinical symptoms and more subtle imaging findings than acute appendicitis and underdiagnosis or delayed diagnosis can lead to complications such as perforation.
- Associated with higher rates of malignancy,
especially carcinoid tumors and mucinous adenocarcinomas.
- When incidentally discovered,
prophylactic appendectomy is recommended.
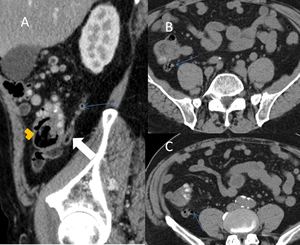
Fig. 19: (A) CT sagittal view of the cecum (orange arrowhead) with a retrocecal appendix (white arrow). A small appendiceal diverticulum (blue arrows) is visualized on the sagittal view and can be better seen on the axial views (B&C)
COLONIC DIVERTICULUM
Colonic diverticula are acquired pulsion diverticulum traditionally thought to be a disease of Western societies secondary to low fiber diets.
In populations with traditionally high-fiber diets, colonic diverticulum affect less than 0.2% of patients. Given the widespread use of screening colonoscopy in the United States,
disease burden can be classified endoscopically by the Diverticular Inflammation and Complication Assessment (DICA).
This system uses number,
extension,
inflammatory signs,
and presence of complications to grade disease burden in an attempt to increase therapeutic efficacy.
-Cecal/Ascending Diverticula
- Uncommon in European and American populations (~1-2%)
- More prevalent in Asian populations (~55-75%).
- Often misdiagnosed as appendicitis given the similar presentation.
- CT is the imaging modality of choice for right lower quadrant pain in adults and can reliably distinguish between acute appendicitis and cecal/ascending colon diverticulitis. Fig. 20
- More commonly present with diverticular bleeding.
- While right-sided diverticulitis is often managed medically,
evaluation for underlying adenocarcinoma is important in older patients.
-Descending/Sigmoid Diverticula
- Most common diverticula of the GI tract
- Exceedingly common in European and American populations
- Incidence increases with age,
affecting approximately 50% of the population by age 50,
and 70% of the population by age 80.
Acute diverticulitis is the most common complication with predisposing factors including obesity,
smoking,
sedentary behavior,
and some medications.
Mild cases of left lower quadrant pain in the appropriate age group is often managed as presumed diverticulitis and treated empirically with oral antibiotics.
When symptoms are more severe or do not respond to empiric therapy,
CT is again the diagnostic modality of choice to confirm the diagnosis and assess for disease complications.
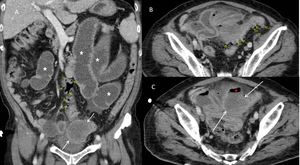
Fig. 21: CT sagittal and axial images showing extensive diverticular disease of the sigmoid colon (yellow arrows) with complicated sigmoid diverticulitis (Hinchey stage 1). There is a developing pericolic abscess (white arrows in images A&C) superior to the bladder dome containing free air (red star). There is a reactive ileus with multiple loops of dilated small bowel (white stars).
Most diverticulitis is uncomplicated,
with imaging features that often include peridiverticular fat stranding,
reactive fluid,
hyperemia in the affected part of the colon,
fluid distention of the colon,
and occasionally a reactive ileus.
Complicated diverticulitis involves larger perforations resulting in local or regional abscesses,
purulent peritonitis,
or feculent peritonitis.
Complicated diverticulitis can be further characterized by the Hinchey or modified Hinchey classification systems as described in Table 1 below.
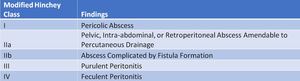
Table 1: Modified Hinchey Classification of Complicated Diverticulitis of the Colon
References: Adapted From: Klarenbeek BR, de Korte N, van der Peet DL, Cuesta MA. Review of current classifications for diverticular disease and a translation into clinical practice. International journal of colorectal disease. 2012; 27(2):207-214.
Accurate characterization of diverticulitis is fundamental to determining treatment approach.
The most advanced cases often require open,
multistage surgery with an initial Hartmann’s procedure and ostomy reversal several months after symptoms and inflammation have resolved.





 on CT sagittal image.")
on fluoroscopy.")
 on CT axial image (A) and CT coronal image (B).")
 and MR maximum intensity projection (B) images. Yellow arrows indicate a small periampullary diverticulum and the gray arrows indicate a large diverticulum along the third portion of the duodenum.")
 on flouoscopy.")
. There is fat stranding around a small hyperdensity (red arrow) which represents an obstructive fecalith.")