Procedure details: The patients we present were admitted to the emergency department for evaluation in an acute setting and the vascular compression syndromes where incidental findings.
Scanning was performed with a 16-slice CT scanner,
intravenous contrast was administered in most cases and MPR,
MIP and 3D reconstructions aided in identifying these entities.
We report cases of Eagle syndrome,
nutcracker and posterior nutcracker syndrome,
median arcuate ligament syndrome,
ovarian vein syndrome,
May-Thurner syndrome etc.
Imaging Findings:
A)Compression of a vascular structure
1.Eagle syndrome is due to elongation of the styloid process or calcified stylohyoid ligament.
It can be unilateral but is also often bilateral.
Approximately 4% of the population has an elongated styloid but only 4-10% of them have symptoms related to this finding because of cranial nerve or carotid artery compression.
The cause is unknown but in some cases it is linked to processes causing heterotopic calcification such as abnormal calcium/phosphorus metabolism and chronic renal failure.
CT demonstrates the elongated styloid process which is longer than 3 cm.
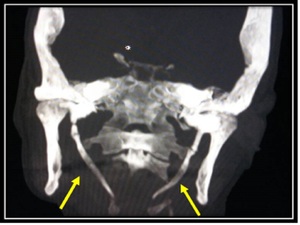
Fig. 1: CT/Coronal plane- MIP image: Asymptomatic patient with demonstration of bilaterally elongated styloid processes. Eagle syndrome
References: Radiology Department “Evangelismos” General Hospital of Athens
2.Nutcracker and posterior nutcracker syndrome: On imaging there is evidence of compression of the left renal vein between the superior mesenteric artery (SMA) and aorta in nutcracker syndrome.
A reduced aortic-SMA angle is also present (the normal angle approximately 45°).
There is also left renal vein stenosis and in some cases thrombosis as a complication,
as well as collateral pathways involving most commonly the left gonadal vein.
Pelvic congestion syndrome may be an additional finding.
Moreover when the compression ratio (diameter of pre-compressed vein minus diameter of compressed vein divided by the diameter of the compressed vein) is over 2.25 this is highly specific for Nutcracker syndrome.
In some case there is compression of a retroaortic left renal vein between the aorta and spine and this is termed as the posterior nutcracker.
The most common clinical finding is recurrent macroscopic hematuria.

Fig. 2: CT image/Axial plane–iv contrast medium administration: This patient presented with hematuria. In this image there is evidence of compression of the left renal vein between the SMA and the aorta with a reduced aortomesenteric distance. Nutcracker syndrome
References: Radiology Department “Evangelismos” General Hospital of Athens
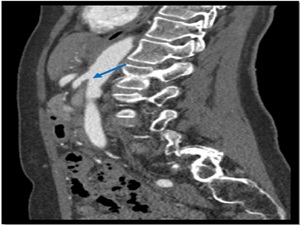
Fig. 3: Same patient (as in figure 2)/Sagittal plane–after iv contrast media administration: small angle between SMA and aorta. Nutcracker syndrome
References: Radiology Department “Evangelismos” General Hospital of Athens

Fig. 4: CT image/Axial plane–iv contrast medium administration: This patient also presented with hematuria. This image illustrates the compression of a retroaortic left renal vein between the aorta and spine. Posterior Nutcracker syndrome
References: Radiology Department “Evangelismos” General Hospital of Athens

Fig. 5: CT image/Axial plane–after iv contrast medium administration: This image illustrates a circumaortic left renal vein with compression of the posterior branch between the aorta and spine in a asymptomatic individual. Posterior Nutcracker phenomenon
References: Radiology Department “Evangelismos” General Hospital of Athens
3.Median arcuate ligament syndrome: Imaging findings (CTA,
MRA and conventional angiography): include focal stenosis-indentation of the celiac artery caused by the median arcuate ligament of the diaphragm.
The celiac trunk obtains a characteristic hooked appearance.
This finding may be evident in normal individuals when scanned in expiration so it is essential that imaging should be performed in the inspiratory phase.
Furthermore there is post stenotic dilatation,
thickening of the arcuate ligament (> 4mm) and collaterals (gastroduodenal and common hepatic arteries).
Clinical manifestation: most patients are asymptomatic,
while others experience weight loss and chronic abdominal pain,
especially postprandial.
Pain is relieved when standing and deteriorated when the patient is in supine position.

Fig. 6: CT image-Sagittal plane after ivc with evidence of compression of the celiac trunk by the median arcuate ligament. Notice the hooked appearance of the celiac trunk. Median arcuate ligament syndrome
References: Radiology Department “Evangelismos” General Hospital of Athens
4.May-Thurner (Cockett) syndrome: Imaging findings: the left common iliac vein is compressed between the fifth lumbar vertebrae and the right common iliac artery.
Additional findings include deep vein thrombosis (DVT) due to stasis from compression and pulmonary embolism.
Clinical presentation: Unilateral (left) lower extremity edema and pain,
varicose veins,
DVT or venous ulcers.
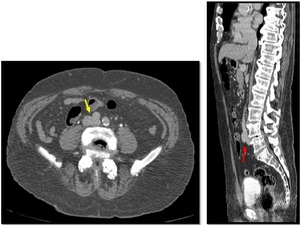
Fig. 8: On the left: CT image in axial plane after ivc The left common iliac vein is compressed by the right common iliac artery. On the right: CT image sagittal plane after ivc administration (same patient). The left common iliac vein is compressed between the right common iliac artery and L4-L5 vertebrae.
References: Radiology Department “Evangelismos” General Hospital of Athens
5.Thoracic outlet syndrome (TOS): Is a group of syndromes which are due to congenital or acquired (anatomic and posttraumatic) compression of the brachial plexus or subclavian vessels at the superior thoracic outlet and therefore TOS is divided into three types the neurogenic (which is the commonest),
venous and arterial TOS.
A combination of neurovascular pathology may also be present.
Imaging must be performed with both arms abducted as well as adducted in order to compare both sides.
Imaging findings include bone and soft tissue abnormalities,
enlarged collaterals (venous or arterial),
vessel narrowing (arterial or venous) with abduction,
arterial aneurysm or pseudoaneurysm,
thrombi (arterial or venous),
distal arterial emboli (in arterial TOS),
edema in brachial plexus (in neurogenic type).
6.Paget Schroetter syndrome: Is a subtype of TOS and is characterized by compression of the subclavian vein in the costoclavicular space with accompanying thrombosis and evidence of arm swelling and pain.
7.Popliteal artery entrapment syndrome: Compression of the popliteal artery by the medial head of gastrocnemius or less commonly popliteus muscle with concomitant diastasis between the vein and artery on imaging.
This syndrome is divided into five types based on anatomical abnormalities.
Patients may present with recurrent claudication,
signs of arterial compromise (when plantar flexion or dorsiflexion),
aneurysm formation,
acute thrombus formation and acute ischemia due to chronic repeated arterial compression in combination with poorly developed collateral vessels.
8.Malignant origin of coronary artery: This a congenital anomaly which is characterized by an abnormal-atypical course of the coronary artery,
which passes retroaortic,
sub or pre-pulmonic in benign types and between the ascending aorta and pulmonary trunk in the malignant form.
In most cases individuals are asymptomatic.
However,
in symptomatic patients it can lead to myocardial ischemia and arrhythmias and can be associated with a risk of sudden death.
B) Compression by a vascular structure
1.SMA syndrome: Compression of the 3rd part of the duodenum by SMA.
Acute presentation includes signs of duodenal obstruction while chronic clinical findings include,
intermittent abdominal pain with vomiting and anorexia.
On CTA and MRA the aortomesenteric angle and distance are reduced and measure approximately 6⁰-15⁰ and 2-8 mm respectively.
There are also findings of dilatation of the 1st and 2nd part of the duodenum as well as collapsed small bowel distally.
2.Nutcracker syndrome
3.May-Thurner (Cockett) syndrome
4.Ovarian vein syndrome: A dilated ovarian vein (more common the right) compresses or obstructs the ureter,
usually due to varicoses of the vein or thrombosis.
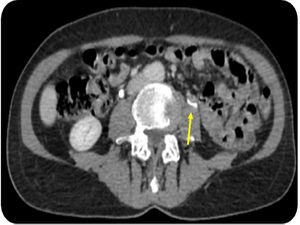
Fig. 9: CT image in axial plane after ivc -excretory phase: Left ovarian vein compressing the ipsilateral ureter. Ovarian vein syndrome
References: Radiology Department “Evangelismos” General Hospital of Athens
5.Innominate artery compression syndrome: An atypical position of the thymus causes diversion of the brachiocephalic artery from its normal position thus resulting in compression-stenosis of the trachea at the level of the thoracic outlet.
This condition occurs in children.
6.Cranial nerve neurovascular compression syndromes:
a) CN V: leads to trigeminal neuralgia which usually lasts a few seconds to two minutes and the most common cause is a loop of an artery (usually the superior cerebellar artery) or vein pressing on the trigeminal nerve at the level of the cerebellopontine angle.
b) CN VII: Causes hemifacial spasm which often begins with painless spasm of the orbicularis oculi and usually spares the frontalis muscle.
It is due to compression of the facial nerve usually by AICA,
PICA and vertebral artery.
7.Aortosternal venous compression: Compression of the brachiocephalic vein between the aorta and the sternum.
Usually patients are asymptomatic.
In case of a symptomatic patient left upper arm and neck swelling are observed.
8.Vertebral arterial loop: Portion of the vertebral artery forms a loop and in some cases it can cause bone erosion,
vertebrobasilar insufficiency and neurovascular compression.
9.Vascular rings:
a)Double aortic arch: Compression of the anterior wall of the trachea and the posterior wall of the esophagus.
It can cause esophageal and/or tracheal obstruction.
Respiratory symptoms are common in infants and swallowing disorders in adults.
Rarely congenital heart disease coexists.
b)Left arch with aberrant right subclavian artery Causes indentation of the posterior wall of the esophagus and results in dysphagia lusoria.
c)Right arch with aberrant left subclavian artery: Causes indentation of the posterior wall of the esophagus.
d)Pulmonary sling/Aberrant left pulmonary artery: The left pulmonary artery arises from the right pulmonary artery and then courses between the trachea and the esophagus in order to end up in the left lung.
This process may cause compression of the posterior wall of the trachea and the anterior wall of the esophagus.
Additional findings on imaging include horizontal course of the main bronchi and in some cases atelectasis of the upper lobes.
Respiratory symptoms predominate.



/Sagittal plane–after iv contrast media administration: small angle between SMA and aorta. Nutcracker syndrome References: Radiology Department “Evangelismos” General Hospital of Athens")




. The left common iliac vein is compressed between the right common iliac artery and L4-L5 vertebrae. References: Radiology Department “Evangelismos” General Hospital of Athens")
