The spinal dural sleeve is a thick,
vascularized connective tissue layer that extends from the foramen magnum,
to the filum terminale and continues along the filum to the coccyx[1].
The rostrally fusion of spinal and periosteal layers of dura mater at foramen magnum prevents its’ intracranial extension [2].
Laterally the dura continues outward around the nerve roots as the dural root sleeves [1].
The epidural or extradural spinal space,
which is space between the dura mater and the bony spinal canal [3],
is a potential space that extends from the foramen magnum to the sacrum.
It is divided into divide into anterior,
lateral and posterior compartments by anchoring plicae and meningovertebral ligaments [4].
Posteriorly,
it’s the space between the dura and the ligamentum flava and periosteum of the vertebral bodies,
pedicles and laminae and it is most ample at the upper thoracic levels [4].
Anteriorly,
the dura is fused with the posterior longitudinal ligament and the annular ligament at the level of each intervertebral disc.
It contains fat tissue-predominantly on the its posterior component,
spinal nerves,
epidural veins and arteries.
The epidural space communicates freely with the paravertebral space via intervertebral foramina [3].
Common signs and symptoms of epidural space lesions are related to spinal cord or radicular compression.
MRI is the gold standard for spine imaging [4].
Its superior soft tissue visualization and contrast differentiation between normal and pathologic tissues allow early diagnosis and accurate anatomic localization of the lesion [1].
But spinal CT is frequently the first imaging method,
especially in an emergent or trauma situation.
CT scan can elucidate a space occupying lesion,
particularly it has a hemorrhagic component,
into the spinal canal.
It is also a great method providing information on the bony spinal components [1].
Epidural space lesions arise from outside the dura mater and can be grouped into intrinsic (arising primarily on the epidural compartment) and extrinsic (secondarily involving the epidural compartment).
In both groups infectious,
benign and malign neoplasms,
traumatic,
degenerative and miscellaneous lesions can be found (Fig.
1)
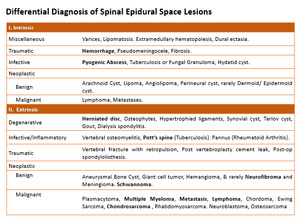
Fig. 1: Differential diagnosis of epidural spine lesions
References: © Chhabra A et al. Spinal epidural space: Anatomy, normal variations and pathological lesions on MR Imaging. Neurographics. Volume 2005 (Issue 1:26):1–13).
