1. How to diagnose Ground Glass opacities?
Focal GGO appear as “hazy increased opacity of lung,
with preservation of bronchial and vascular margins. »(1) (Fig.1).
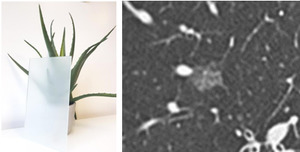
Fig. 1: Focal Ground glass opacities
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Diffuse GGO are sometimes more difficult to identify because of the lack of normal parenchyma: In this case,
comparing parenchyma’s density,
to air density in the bronchiole can help us make the diagnosis.
(Fig.
2).
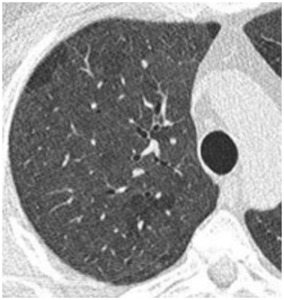
Fig. 2: Diffuse Ground glass opacities
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Pay attention to pitfalls!!!
- Mind expiratory acquisitions which may lead to wrong diagnosis of GGO (2): It’s important to always check the shape of the trachea.
The posterior membranous wall of the trachea is flattened or bowed inward during expiration.
(Fig.
3)
- Mind position-dependent GGO (posterior regions) (2).
(Fig.
4)
- Always check if the patient recently had a bronchoalveolar lavage because it can mislead the diagnosis
- Mosaic oligemia and perfusion (2): It’s a « patchwork of regions of differing attenuation » (1).
Distinguishing this pattern from GGO is based on the comparison of vessels’ diameter and number.
If they are comparable in the different region,
it’s a ground-glass opacity.
When vessels are smaller and rarer in the hypodense regions,
It’s a mosaic oligemia and perfusion.
(Fig 5).
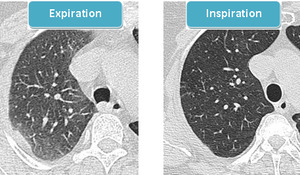
Fig. 3: Expiratory GGO: the posterior wall of the trachea is bowed inward during expiration. “GGO” disappear when we repeat the scan during inspiration
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
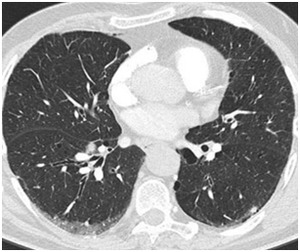
Fig. 4: Positional GGO
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
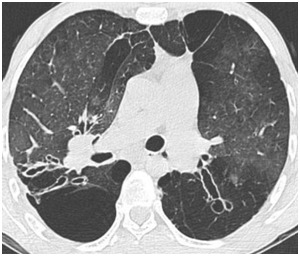
Fig. 5: Mosaic perfusion
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
2.
How to identify Ground-glass opacities’ etiologies?
Two things are important to consider when dealing with GGO (3):
· Clinical manifestations: We will consider here to major situations: acute symptoms Vs.
Chronic symptoms.
Some other informations are also important like hemoptysis,
immune depression,
fever…
· Imaging findings: Focal Vs.
Diffuse GGO / Topography / associated signs…
2.1.
Diffuse and multiple GGO:
2.1.1.
Acute symptoms
Cardiogenic pulmonary edema & Diffuse alveolar hemorrhage:
They have similar aspects on chest CT scans with regular septal thickening and diffuse GGO.
Theses GGO tend to be peri-hilar,
bilateral and symmetric.
History of cardiac disease,
cardiomegaly and bilateral pleural effusion make cardiogenic pulmonary edema more likely (2,3) (Fig.6).
Hemoptysis and history of auto immune disorders are more commonly found in diffuse alveolar hemorrhage (2,3) (Fig.7).
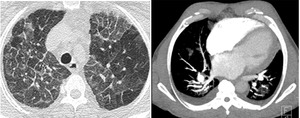
Fig. 6: Pulmonary edema: GGO with regular septal thickening, pleural effusion and cardiomegaly
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
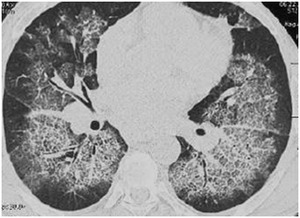
Fig. 7: Diffuse alveolar hemorrhage with central GGO with regular septal thickening
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Acute respiratory distress syndrome (ARDS,
also known as diffuse alveolar damage)
When clinical symptoms are brutal with diffuse or multiple GGO on CT,
an ARDS should be considered,
especially when (3):
- There’s a possible inciting event
- GGO are asymmetric and associated to pulmonary consolidations (Fig.8)
- Fibrosis with traction bronchiectasis appear later
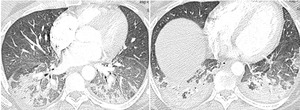
Fig. 8: Diffuse alveolar damage: GGO and pulmonary consolidations
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Hypersensitivity pneumonitis
It’s an interstitial granulomatous pneumonitis in susceptible individuals secondary to exposure to inhaled organic or inorganic particles.
The sub-acute form manifests with centrolobular nodules and GGO,
patchy or diffuse GGO.
Mosaic attenuation with a combination of patchy areas of GGO and air trapping are also common features (2) (Fig.9).
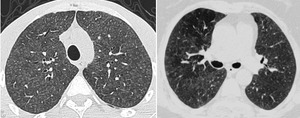
Fig. 9: Hypersensitivity pneumonitis in 2 different patients: The first one shows centrolobular nodules and GGO and the second one shows additional air trapping
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Infectious diseases
In persons with immune suppression the first diagnosis to consider is pneumocystosis. It’s a fungal infection by Pneumocystis jiroveci,
most often in patients with impaired cell- mediated immunity.
It manifests on CT as peri-hilar,
diffuse GGO,
sometimes associated with septal thickening.
It’s immune depression and air-containing thin-walled cysts with an upper lobe predilection that must make the radiologist consider Pneumocystosis (2,3) (Fig.10).
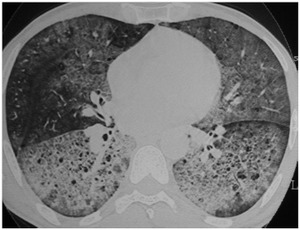
Fig. 10: Pneumocystosis: Diffuse GGO with cysts in a patient with immune suppression
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
2.1.2.
Chronic symptoms
In chronic situations,
most frequent causes are diffuse infiltrative lung diseases and particularly non-specific interstitial pneumonia (NSIP),
smoking related interstitial pneumonias (Desquamative interstitial pneumonia (DIP) &  Respiratory bronchiolitis-interstitial lung disease (RB-ILD)) and lymphoid interstitial pneumonia (LIP) (3).
Respiratory bronchiolitis-interstitial lung disease (RB-ILD)) and lymphoid interstitial pneumonia (LIP) (3).
Non-specific interstitial pneumonia (NSIP):
Presence of symmetric lower lobe predominant peripheral GGO and reticulation should suggest the diagnosis.
Findings of traction bronchiectasis with lower lobe volume loss are additional imaging features that may indicate a fibrotic form of NSIP(2,3) (Fig.11).
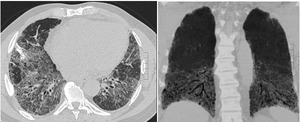
Fig. 11: NSIP: Diffuse GGO mainly in the lower lobes with reticulations and bronchiectasis
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Lymphoid interstitial pneumonia (LIP):
It is an interstitial pneumonia which is associated with autoimmune disorders,
particularly,
Sjögren syndrome,
and immune depression (HIV infection,
bone marrow transplant).
Diffuse GGO is the predominant CT imaging feature of LIP.
Associated thin-walled air cysts and adenomegalies suggest the diagnosis.
Desquamative interstitial pneumonia (DIP):
A history of cigarette smoking is helpful in suggesting DIP.
Its aspect on chest CT scan is close to LIP’s aspect with diffuse GGO with Multiple small cysts.
Absence of immune depression,
signs of smoker’s lungs (emphysema,
bronchial wall thickening) and lesions’ regression with smoking cessation suggest the diagnosis (Fig12).
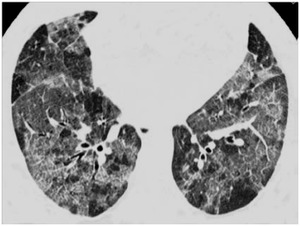
Fig. 12: Desquamative interstitial pneumonia
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Respiratory bronchiolitis-interstitial lung disease (RB-ILD):
It’s also a smoking related interstitial pneumonia.
RB manifests as upper lobe predominant centrolobular GGO and bronchiolar wall thickening.
A smoking history and coexistence of emphysema must make us think of it (2) (Fig.13).
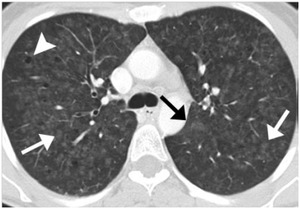
Fig. 13: RB-ILD: Centrolobular nodules and GGO (white arrows), cysts (arrow head) and emphysema (black arrow)
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Veno occlusive disease:
Respiratory signs are rapidly progressive.
CT scan shows pulmonary edema,
regular septal thickening,
pleural effusion,
pulmonary arterial hypertension and mediastinal nodes hypertrophy (Fig14).

Fig. 14: Veno occlusive disease: Centrolobular nodules and GGO, madiastinal lymph node hypertrophy and pulmonary arterial hypertension
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
2.2.
Focal GGO
An ill defined focal GGO can be a focal alveolar hemorrhage or an infection.
Tree in bud nodules and clinical signs will help us narrow the diagnosis of infection.
A follow-up CT in 3 months is also compulsory to affirm the infection.
A persistent ground glass nodule can be an atypical adenomatous hyperplasia. It manifests on CT as a persistent focal well-defined GGO nodule without any solid component,
and without change in size on follow-up CT studies (Fig15). These follow-up studies are very important because atypical adenomatous hyperplasia may transform into malignant tumors.
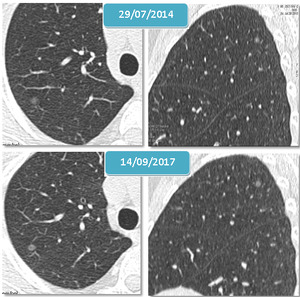
Fig. 15: Atypical adenomatous hyperplasia: Grond glass nodule without solid component, stable in the 3 year control
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Change in size or solid component must ring in the radiologist head as a warning signal.
It may be an adenocarcinoma in situ or a micro invasive adenocarcinoma.In adencarcinoma in situ (Fig.16),
the ground glass nodule doesn’t contain any solid component because there’s no infiltration of the stroma but there’s a lepidic extension near vessel’s wall.
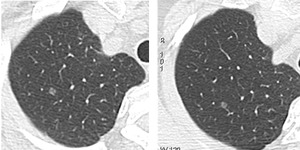
Fig. 16: Adenocarcinoma In situ: Persitent Grond glass nodule without solid component
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
Micro invasive adenocarcinomas manifest with part-solid nodules (Fig.17).
So ,
all ground-glass and part-solid nodules bigger than 6 mm must benefit from a regular surveillance until 5 years (4)(Fig.18).
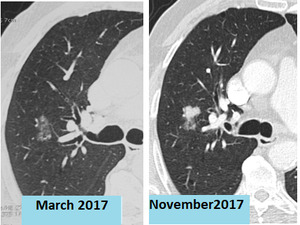
Fig. 17: Micro invasive Adenocarcinoma: Ground glass nodule with minimal solid component. In the 6 month control, there’s a growth of the solid component
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
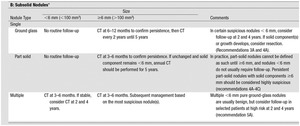
Fig. 18: Fleischner Society recommendations for subsolid incidental nodules detected in CT scans
References: MacMahon H, Naidich D, Goo JM, Le KS, Leung A, Mayo J and al. Guidelines for Management of Incidental Pulmonary NodulesDetected on CT Images: From theFleischner Society 2017. Radiology. 2017;284(1):228-43
2.3.
Particular aspects:
2.3.1.The “Crazy paving”
It’s defined as “thickened interlobular septa and intralobular lines superimposed ona background of GGO.” (1) It can be caused by (2) :
- Pulomnary alveolar proteinosis: The diagnosis is suspected when there’s discordance between severe imaging findings and mild clinical manifestations.
It’s confirmed by bronchoalveolar lavage (Fig.19).
- Pulmonary edema (Fig.20)
- Diffuse alveolar hemorrhage (Fig.21)
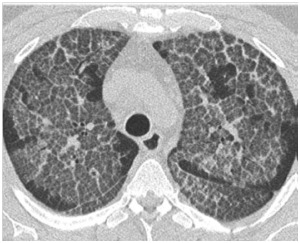
Fig. 19: Crazy paving: Alveolar proteinosis
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia

Fig. 20: Crazy paving: Pulmonary edema
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia

Fig. 21: Crazy paving: Diffuse alveolar hemorrhage
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
2.3.1.
Halo sign
It’s defined as « ground-glass opacity surrounding a nodule or mass » (1).
This sign may be secondary to:
- Hemorrhagic nodules or masses:
o Fungal infections: Invasive aspergillosis: air-crescent sign,
and cavity formation (Fig.22)
o Bacterial infections: Septic emboli
o Hemorrhagic pulmonary metastasis: Angiosarcoma,
choriosarcoma,
and melanoma
o Vascularitis: Wegener granulomatosis
- Inflammatory disorders : cryptogenic organizing pneumonia: Migratory GGO with both “halo sign” and more specifcally “reversed halo sign.
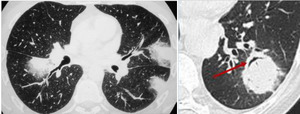
Fig. 22: Invasive aspergillosis in two different patients: The first one shows halo sign during aplasia period and the second one air crescent sign which appears when the patient is no more in aplasia
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
2.3.2.
Particular aspects: Reversed Halo sign
The Fleischner society’s glossary defines reversed halo sign as “focal rounded area of GGO surrounded by a more or less complete ring of consolidation » (1).
The reversed halo sign has been described in a variety of diseases,
such as:
- Cryptogenic organizing pneumonia (Fig.23)
- Invasive aspergillosis
- Wegener granulomatosis
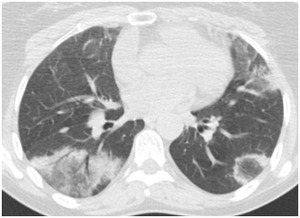
Fig. 23: Cryptogenic organizing pneumonia: Reversed halo
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
3. Tips and tricks to deal with GGO:
To resume all the reflection that we have done,
we propose the following figures (Fig.
24,
25 and 26) to help radiologist identify etiologies of GGO.
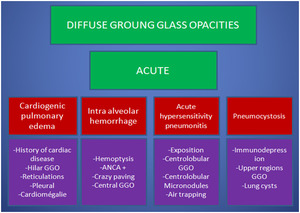
Fig. 24: Tips and tricks to deal with acute & diffuse GGO
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
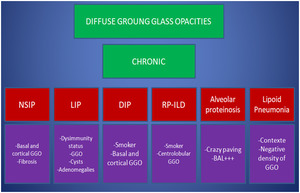
Fig. 25: Tips and tricks to deal with chronic & diffuse GGO
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
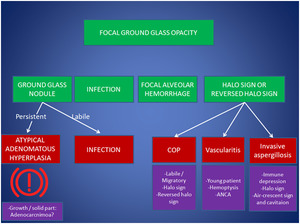
Fig. 26: Tips and tricks to deal with focal GGO
References: Department of Radiology. Abderrahmen Mami Hospital, Ariana, Tunisia
