This pictorial review illustrates the different types of craniosynostosis with cases from our institution using different imaging methods,
including head X-ray and CT scans.
Normal cranial sutures
The human skull is composed by four large sutures (sagittal,
coronal,
lambdoid and squamosal) which separate the primary cranial bones (frontal,
parietal,
occipital and temporal) and persist into adulthood.
There are also minor sutures,
namely the metopic,
sphenosquamosal,
sphenofrontal,
and occipitomastoid sutures,
which are opened in infants and toddlers.[2,6,12] The sagittal suture separates both parietal bones; coronal sutures exist between the frontal and parietal bones; between the parietal and occipital bones there are the lambdoid sutures; and the squamosal sutures lay between the parietal and temporal bones.(Figure1)[11]
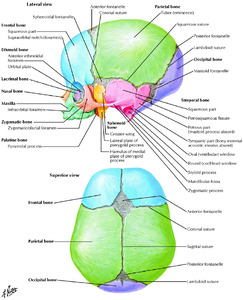
Fig. 1: Skull of the newborn.
References: Netter FH, Dalley AF. Atlas of human anatomy. 2nd ed. East Hanover, NJ: Novartis, 1997.
According to Virshow’s law,
cranial bones grow perpendicular to the suture line,
which fuses from back to front and lateral to medial,
except the metopic suture (fusion from front to back).[10,11,12] Table 1 shows the normal age of closure for the main sutures.

Table 1
Craniosynostosis
This review will address the major sutures craniosynostosis,
since those are more often affected.
The number,
order and extent of suture involvement result in different calvarium deformities,
which are summed up in Table 2.[4]
Table 2
a) Sagittal synostosis
Sagittal synostosis is the most common type of simple craniosynostosis,
accounting for more than half of all the cases,
and its incidence is 1-2.5 in 5000 live births.[6,13,14] Its prevalence is four times higher in males.[2,4]
The premature fusion of the sagittal suture leads to the restriction of biparietal growth (perpendicular to the suture),
which results in a compensatory antero-posterior growth (along the suture).
The cranium becomes elongated and narrow,
with a reduced cephalic index (ratio between the biparietal and the antero-posterior diameters),
hence the use of descriptive terms like dolichocephaly (Greek: dolikhos = long) or scaphocephaly (Greek: scaphe = boat).[2,4,6]
Lateral plain skull radiograph is frequently diagnostic,
showing the fused sagittal suture and anterior fontanel,
as well as the characteristic head shape.[2,4] These changes are also evident on the CT-3D,
which is useful in treatment planning.(Figure2)
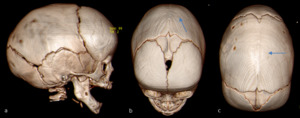
Fig. 2: Scaphocephaly in a 7-months-old boy. Lateral (a) CT-3D shows a skull elongation. Anterosuperior (b) and superior (c) CT-3D views show the fused sagittal suture (arrows).
Surgical repair,
either by a traditional open procedure or by an endoscope-assisted craniectomy,
is the treatment of choice.[2,13]
b) Coronal synostosis
Unicoronal synostosis is the second most common type of craniosynostosis and its prevalence is higher in females.[2,6,10] The head deformity is called anterior plagiocephaly (Greek: plagios = oblique),
since there is an asymmetry of the anterior cranial fossa because the antero-posterior growth on the affected side is restricted.
That restriction is responsible for an ipsilateral Harlequin-eye deformity (orbital roof and lesser wing of the sphenoid superiorly displaced) and a flattening and posterior displacement of the calvarium.
On the contralateral side,
there is a compensatory overgrowth with anterolateral bossing of frontal and parietal bones.
Together,
these changes result in a trapezoid shape of the head,
if seen from above.(Figures 3,4)[2,14] Treatment is surgical.
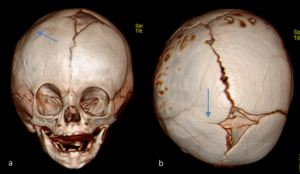
Fig. 3: Anterior plagiocephaly in a 5-months-old girl. Frontal (a) and superior (b) CT-3D views show the prematurely fused right coronal suture (arrows). Orbit assymetry is also noted (a) and the calvarium has a trapezoid shape (b).
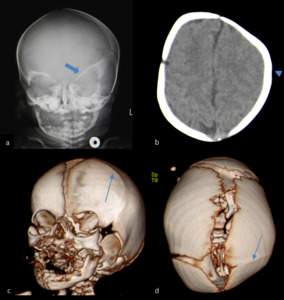
Fig. 4: Anterior plagiocephaly in a 20-days-old girl. The plain skull radiograph taken 3 days after birth (a) shows a Harlequin-eye deformity on the left (thick arrow). Axial non contrast CT image (b) shows a fused left coronal suture (arrow head), which is seen in anterolateral and superior CT-3D views (c,d) as a proeminent ridge (thin arrows). All the other sutures are unfused, as expected for the age.
Premature fusion of both coronal sutures is described as brachycephaly (Greek: brakhu = short) and is commonly associated to genetic syndromes,
such as Apert,
Crouzon or Saethre-Chotzen.[1,4,6] The skull has a short antero-posterior diameter but a compensating biparietal growth,
resulting in a high cephalic ratio.
The frontal bone is protuberant,
the occipital bone is flattened,
and usually there is bilateral Harlequin-eye,
which can be identified on the CT-3D,
along with the bicoronal synostosis and the fused anterior fontanel.(Figure5) The plain skull radiograph is sufficient to detect the fused sutures and the orbit deformity,
making the diagnosis,
but CT and MRI are more useful for evaluation of associated anomalies.
Surgery should be performed with a fronto-orbital advancement procedure.[2,4,10]
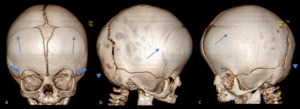
Fig. 5: Brachicephaly in a 6-months-old girl. Anterosuperior (a), lateral (b) and anterolateral (c) CT-3D views demonstrate premature fusion of both coronal sutures (arrows), which creates a short cranium. Frontal bossing and bilateral Harlequin-eye deformity (thick arrows) is also seen. The occipital bone is flattened (arrow head).
c) Metopic synostosis
The fusion of the metopic suture before the age of 6 months is associated to trigonocephaly (Greek: trigonos = three angles),
given the triangular appearance of the anterior calvarium.
There is a narrowing of the anterior cranial fossa,
leading to a pointed forehead,
and a compensatory growth of the middle cranial fossa with bossing of the parieto-occipital regions.
It is associated with other midline abnormalities and is syndromic in one-third of the cases.[1,2,10]
The diagnosis may be clinical and is confirmed with a plain skull radiograph or CT-3D.
These imaging modalities show the typical triangular shape of the head with the fused metopic suture.
On the CT-3D is possible to identify an ectocranial ridge along the suture and a metopic notch,
or an elongated unfused anterior fontanel.(Figure6) There is also hypotelorism,
lateral orbital hypoplasia and hypoplastic ethmoid sinuses.[4,10]
This type of synostosis is highly correlated to neurodevelopmental delay and it remains unclear if surgical treatment corrects it.[15]

Fig. 6: Trigonocephaly in a 11-months-old boy. Frontal (a) CT-3D view shows a fused metopic suture, along with the bulge of the parietal regions. The characteristic triangular shape is evident on the superior (b) and anterolateral (b) views.
d) Lambdoid synostosis
The premature closure of the lambdoid suture is the rarer type of simple craniosynostosis.
It can be unilateral,
causing posterior plagiocephaly,
or bilateral,
resulting in a tall cranium described as turricephaly (Greek: turri = tower),
which is even rarer.[6,15]
Posterior plagiocephaly caused by unilateral lambdoid synostosis is clinically obvious,
due to the characteristic trapezoid skull shape associated to a deformity of the posterior cranial vault – the ipsilateral occipital and parietal bones are flat and the contralateral occipital,
parietal and frontal bones protrude.(Figure7) When both lambdoid sutures fuse prematurely,
the posterior fossa does not develop,
resulting in flat occipital and both parietal bones.
The cranium growths at the bregma and becomes tall with a short antero-posterior diameter.[4,10] Release of the fused suture is achieved with various surgical techniques.[15]
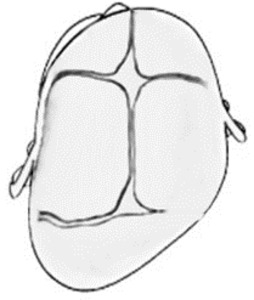
Fig. 7: Schematic representation of posterior plagiocephaly (superior view), caused by the premature fusion of the right lamboid suture.
e) Multisutural synostosis
Complex synostosis is rare and frequently syndromic.
Depending on the affected sutures,
there are different calvarium deformities (Table2 and Figure8).
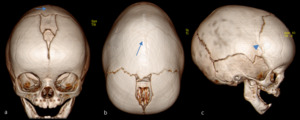
Fig. 8: Complex synostosis in a 8-months-old boy. Anterosuperior (a) and superior (b) CT-3D views demonstrate a prematurely fused sagittal suture (arrows), responsible for the predominant dolichocephaly. On the lateral view (c) the right coronal suture is starting to ossify (arrow head). This is a case of a nonsyndromic craniosynostosis.
The most severe form of craniosynostosis occurs when sagittal,
bicoronal and bilambdoid sutures fuse prematurely,
resulting in a tall and narrow skull with bossing frontal and temporal regions,
shallow orbits and posterior flattening.(Figure9) This trilobar appearance of the skull is known as Kleeblattschädel or cloverleaf and is associated to severe neurological disabilities.[4,10,16]
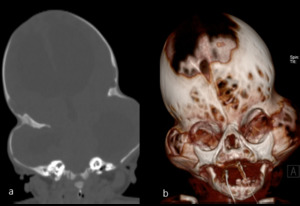
Fig. 9: Kleeblattschädel skull in a 2-months-old boy with Pfeiffer syndrome. Coronal non contrast CT image (a) shows a tall cranium (turricephaly) with bossing temporal regions. Fusion of the metopic and bicoronal sutures, as well as areas of non ossification (characteristic of the syndrome) are seen in frontal CT-3D view (b).
References: Case courtesy of Dr Ian Bickle, Radiopaedia.org, rID 35578
