TR-MRA delivers vascular imaging with enough temporal resolution to assess contrast flow dynamics in arteries and veins (and requiring only a small contrast dose).
A typical TR- MRA study may contain more than twenty images obtained at rates as rapid as 1-5 frames per second.
As we all know (and suffer),
spatial and temporal cannot usually be obtained at the same time.
TR-MRA techniques balance this,
using a process called view-sharing.
Remember the distribution of the k-space: The center of the k-space represents the information about image contrast,
whereas the periphery encodes edge and details of the final image.
Thus,
TR-MRA techniques during the passage of the contrast bolus sample the center of k-space (image contrast) much more frequently than the periphery (edge and details),
which is updated only partially in every acquisition.
The data from the different partial k-space samplings are combined to create a series of images with enough spatial resolution.
For instance,
TR-MRA TWIST technique (implemented by Siemens) uses a random scheme.
During TWIST acquisition,
the center (C) is always filled completely.
It is in this area that one expects the greatest changes in contrast due to the inflow of contrast agent.
Periphery (P) is also completely covered in a single measurement,
but it is sampled with a reduced density.
As a result,
multiple passes through P are required to obtain the data with full density.
However,
missing points in k-space can be supplemented from previous or future measurements of P to calculate a complete 3D MRA data set at any time.
When planning the sequence user must choose the size of region C (usually 15-30% of the entire k-space),
the undersampling rate in the P region (usually 20-30%) and the number of frames that are adequate to the circulation time in the area of interest or pathology studied.
For instance,
with 30% for the size of region C and 25% for the undersampling in P,
the TWIST acceleration is 2.1,
i.e.
the TWIST acquisition provides a 2.1-fold acceleration over a conventional acquisition using similar measurement parameters.Adding the values for parallel imaging and partial Fourier,
the total acceleration increases to 9.8.
In other words,
the acquisition is nearly 10 times faster than a standard,
full k-space acquisition technique.
All time-resolved MRA methods have at their core a 3D-spoiled GRE sequence with thin slices,
very short TRs and TEs,
low flip angles, use of both read- and phase-conjugate symmetry,
parallel imaging acquisition,
and zero-interpolation filling in the slice direction. Most sequences start using a mask (a full-resolution image) prior to the arrival of the contrast bolus,
so subtracted images can be obtained.
Gadolinium is power injected at a usual rate of 2-3 ml/s.
Accurate timing of bolus arrival is not required (shoot and forget technique!).
The technologist simply starts the sequence and runs it until the contrast has passed through the vascular system.
A smaller dose of contrast can also be used than with conventional CE-MRA due to the higher conspicuity.
Clinical utility of TR-MRA by anatomical region:
TR-MRA is a very useful sequence for evaluation of
-high flow vascular beds
-sites of non-predictable contrast arrival time
-arteriovenous malformations
-collateral and retrograde flow at sites of vascular stenoses.
Head and Neck:
Evaluation of arteriovenous malformation (AVM) and dural fistulae
Supra-aortic arteries atherosclerotic disease of the supraaortic arteries without venous contamination
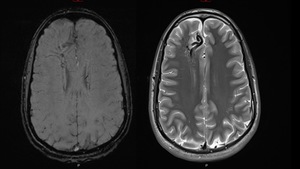
Fig. 3: Complex vascular malformation consisting of prominent and tortuous venous vascular structures that show signal emptying in T2-weighted sequences due to high flow
References: Servicio Radiodiagnóstico, Clínica Universiaria de Navarra
Fig. 4: TR-MRA shows high flow with dynamic filling of the collecting vessels at the same time time than the longitudinal venous sinuses.
References: Servicio Radiodiagnóstico, Clínica Universiaria de Navarra
Fig. 5: Surrounding parenchyma of the frontal lobe shows a great vascular plume with multiple venous thin vessels that adopt a morphology in a caput medusae sign.
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
Thorax:
Cardiac: integrity of postoperative shunts and conduits
Aorta: dissection,
aneurysm
Pulmonary vessels
Central Veins
Abdomen and Pelvis:
Native and transplanted abdominal and pelvic organs and their vasculature
Pelvic congestion
Penis
Fig. 6: Patient with chronic liver disease. Previous US imaging arose suspicion for hepatic arterioportal shunt. TR-MRA confirmed no shunt was present.
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
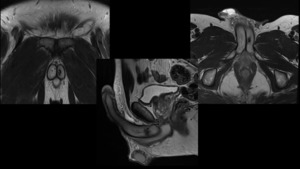
Fig. 7: Patient with ED after a blunt trauma affecting the penis. MRI depicts hypointense and irregular area of 9 mm in T2 weighted image, located in the posterior portion of the left corpus cavernosum, corresponding to fibrous tissue.
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
Fig. 8: TR-MRA depicts early enhancement of left corpus cavernosum, arising from left internal pudendal artery. The findings are compatible with arteriovenous fistula, secondary to previous trauma.
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra

Fig. 9: TR-MRA depicts early enhancement of left corpus cavernosum, arising from left internal pudendal artery. The findings are compatible with arteriovenous fistula, secondary to previous trauma
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
Extremities:
Thoracic outlet syndrome
Raynaud’s disease
Popliteal artery entrapment syndrome.
AVM and vascular
hemodialysis grafts/fistulas



