The inguinal region is a complex area,
intersecting multiple structures that form a short and narrow passage in the lower abdominal wall,
lined by the aponeuroses of the external oblique,
internal oblique and transversus abdominis muscles.
The structures that cross the inguinal canal are different depending on gender,
so some pathologies are specific and should be suspected,
when in the proper clinical context.
A variety of nonneoplastic and neoplastic masses can be found in the inguinal region,
and the identification of certain characteristic imaging features,
along with clinical information,
may help in narrowing the differential diagnosis.
Imaging methods like ultrasound,
computed tomography (CT) and magnetic resonance (MR) imaging,
play an important role in this assessment.
Anatomy of the inguinal canal
The inguinal canal (IC) is an oblique inferomedially directed ~4cm passage that is lined by the aponeuroses of three abdominal wall muscles: the external oblique,
internal oblique,
and transversus abdominis muscles.
These abdominal wall muscles compose the anterior and posterior walls,
roof,
and floor of the IC (figure 1).
The IC contains blood and lymph vessels,
the ilioinguinal nerve,
the spermatic cord in male and the round ligament in female individuals.
The spermatic cord goes from the pelvic cavity to the scrotum and includes the lymphatic vessels,
the ductus vas deferens,
the testicular,
cremasteric and deferential arteries and veins (pampiniform plexus),
and the genital branch of the genitofemoral nerve.
In females,
the IC carries the round ligament of the uterus and the ilioinguinal nerve to the labia majora[1,2].
The IC has two openings: the superficial inguinal ring,
which has an inverted 'V' shaped,
located in the medial end of the external oblique aponeurosis,
above and lateral to the pubic tubercle (figure 1 A),
and the deep inguinal ring,
which is an anatomic defect in the transversalis fascia,
located laterally by the angle between the transversus abdominis muscle and inguinal ligament,
and medially to the inferior epigastric vessels (figure 1 B).
The inferior epigastric vessels that arise from the external iliac artery and vein immediately above the inguinal ligament (figure 1 B),
represent an essential anatomical point,
particularly on ultrasound,
allowing to locate the deep inguinal ring,
and consequently the related pathology[1].
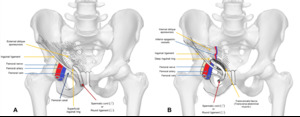
Fig. 1: Illustration of normal anatomy of the inguinal region (anterior view). A) Inguinal canal with the external oblique aponeurosis intact; B) Inguinal canal without the external oblique aponeurosis, showing deep inguinal ring and transversalis fascia.
