The initial evaluation of inguinal canal (IC) after physical examination,
usually begins with ultrasound,
since IC is superficial and easy to study by this method.
Ultrasonography allows imaging in real time,
at rest or using dynamic patient maneuvers that can be optimized based on the suspected pathology.
So,
it is essential to know the types of probe to be used (usually high-frequency linear transducers) and the correct positioning of the probe to obtain the appropriate plans,
based on the anatomical points of reference.
In some patients,
it may be crucial to acquire images from the contralateral side of the complaints,
for comparative purposes.
On ultrasonography (figure 2),
the IC is seen as a linear structure with a double contour whose normal thickness is approximately 4 mm.
To assure a correct evaluation of the IC,
it is important to avoid channel compression during the examination.
Sometimes the ultrasound evaluation is insufficient,
so in these cases,
CT and MRI may reveal crucial additional information,
especially if the intra-abdominal extent of the process needs to be assessed.
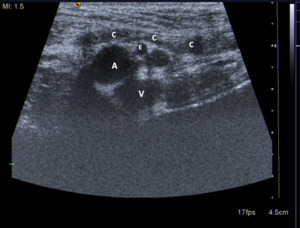
Fig. 2: Sonogram of the inguinal region parallel to inguinal ligament shows spermatic cord (C), external iliac artery (A), inferior epigastric artery (E) and femoral vein (V).
Benign pathology affecting the Inguinal Canal
A) Inguinal Hernia
Inguinal hernias are a protrusion of the intra-abdominal structures to the IC,
and represents the commonest type of abdominal wall herniation and are most often acquired[5].
There are two main types of inguinal hernias: the indirect type,
accounting for about 50% of all inguinal hernias,
and the direct type,
which represents up to 25% of these protrusions[1].
Although femoral hernias are also considered groin hernias,
they do not affect the IC,
so they will not be discussed in detail in this poster.
The indirect type occurs when the abdominal contents pass through the deep inguinal ring into the inguinal canal.
In this case,
the contents of the hernia can cross the superficial ring and descend into the scrotum or labia majora.
Indirect inguinal hernias are more common in men and are considered to be congenital[1].
Direct inguinal hernias are not congenital and occur when the abdominal contents enter the IC through a defect in the aponeurosis of the posterior wall of the IC.
They are commonly bilateral and tend to affect older individuals as a result of relaxation of the abdominal wall musculature and thinning of the fascia[1,4].
Complications of inguinal hernias,
as in any other abdominal wall herniation,
include incarceration,
strangulation and bowel obstruction.
Ultrasound (US) assessment may be crucial in the distinction between these two types,
and figure 3 illustrates the position of the transducer for the correct evaluation of indirect inguinal hernia,
direct inguinal hernia,
and femoral hernia,
according to their different locations.
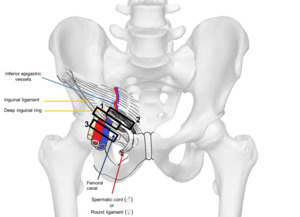
Fig. 3: Illustration of right inguinal region from anterior view shows transducer position to evaluate for indirect inguinal hernia (1), direct inguinal hernia (2) and femoral hernia (3).
During the ultrasound evaluation of the IC,
it is essential to ask the patient to increase abdominal pressure (Valsalva maneuver) to identify transient hernias,
which reduce entirely at rest.
Besides,
the characteristic movement of hernia tissues often confirms the diagnosis.
The typical movement of the hernia content with the Valsalva maneuver may not be detected if the patient is unable to perform the maneuver properly or if the hernia contents are incarcerated[1].
The contents of the hernial sac are variable: omental fat (figure 4),
small bowel (figure 5 and 6),
mobile segments of the colon,
bladder (figure 7),
among others. At US,
if the content is only fat,
it will appear hyperechogenic (figure 5); if the sac contains intestinal loops (figure 6),
it is vital to assess the reducibility and intestinal viability identified by peristalsis or mucosal blood flow.
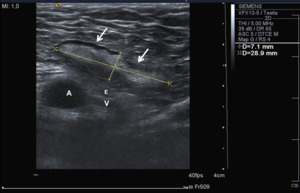
Fig. 4: Ultrasound image of the inguinal region showing an indirect inguinal hernia containing only fat on the inguinal canal.
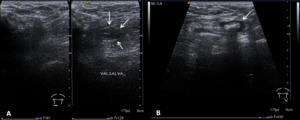
Fig. 5: Ultrasound images of the inguinal region showing: A) a transient inguinal hernia (after Valsalva maneuver) containing a small bowel loop on the right inguinal canal; B) an inguinal hernia containing a small bowel loop on the left inguinal canal.
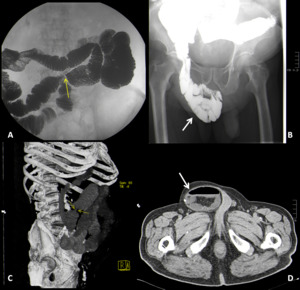
Fig. 6: Small bowel barium study (A and B) shows focal stenosis with substantial reduction of its caliber and a large right inguinal hernia with small bowel loops and fat. CT findings in the same patient (C and D).
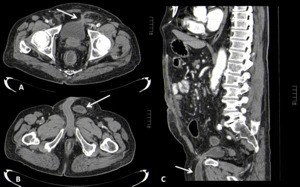
Fig. 7: Axial (A and B) and Sagittal (C) contrast-enhanced abdominal CT images showing an inguinal hernia containing part of the bladder, in an 80 years-old man.
B) Inflammatory or Infectious Processes
Corditis is an inflammation of the spermatic cord.
In man,
the spermatic cord is the main constituent of IC and when it is inflamed or infected,
may cause a painful inguinal mass.
Corditis usually results from retrograde dissemination of pathogens from the prostatic urethra,
prostate,
or seminal vesicles.
On ultrasound,
common findings include increased spermatic cord size with a distended IC,
masslike aspect of the echogenic fat,
and hyperemia during color Doppler evaluation,
which does not change with Valsalva maneuver (figure 8)[1].
In critical cases,
it can lead to vascular compromise and testicular infarction,
due to compression of adjacent vessels.
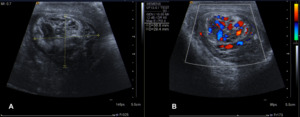
Fig. 8: A) Ultrasound images of the inguinal canal showing corditis of the left spermatic cord with hyperechogenicity of the surrounding fat and increased spermatic cord diameter. B) Increased vascularity at color Doppler study, which is consistent with the inflammatory process.
Fournier gangrene is a necrotizing fasciitis that affects the perineal,
genital and perianal regions,
and therefore may involve the inguinal canal.
It is a real surgical emergency because it is rapidly progressive and has a potentially high mortality rate[6].
The diagnosis of Fournier Gangrene is clinical,
and imaging studies,
such as CT,
allow accurate evaluation of the extent of the disease,
assessing the perineal and retroperitoneal structures that may be involved.
The hallmark of Fournier's gangrene is the presence of subcutaneous emphysema,
which does not appear in all patients but may be noted by ultrasound (figure 9 A and B) or CT (Figure 9 C and D).
Other CT findings include asymmetric fascial thickening,
fluid collections,
and local abscesses[6].
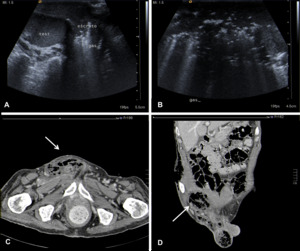
Fig. 9: Ultrasound images of the inguinal region (A and B) and Axial (C) and Coronal (D) contrast-enhanced abdominal CT images showing subcutaneous emphysema in a patient with Fournier gangrene affecting the right inguinal canal and the scrotum.
(Test = testis; Escroto = scrotum; Gas = subcutaneous emphysema)
Causes of abscesses in IC are variable,
such as incarcerated inguinal hernia,
diverticulitis or intravenous drug use.
Clinically there is an irreducible inguinal mass,
fever,
and leukocytosis,
but sometimes the symptoms are nonspecific,
leading to delayed diagnosis. At CT,
the abscesses are masses of low attenuation with ring enhancement (Figure 10).
At MR imaging,
abscesses generally have low signal intensity on T1-weighted images and high signal intensity on T2-weighted images and may exhibit a thin rim of peripheral enhancement[2].
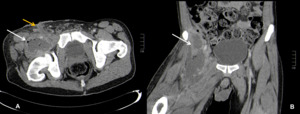
Fig. 10: Axial (A) and Coronal (B) contrast-enhanced abdominal CT images showing a local abscess (white arrows) in a 36-year-old drug user. Yellow arrow shows the drainage path to the skin.
C) Lesions of vascular origin
- Femoral artery pseudoaneurism
Pseudoaneurysm occurs when there is a breach in the vessel wall such that blood leaks through the wall but is contained by the adventitia or surrounding perivascular soft tissue.
Femoral artery pseudoaneurysms are usually iatrogenic after endovascular arterial interventions and other causes are intravenous drug use or penetrating trauma[7].
Ultrasound is the modality of choice for assessment,
showing the characteristic yin-yang sign (also known as Pepsi sign) in color Doppler (figure 11 A),
which happens due to the turbulent/bidirectional flow into the false aneurysm[8].
On CT (figure 11 B) the patent portion of the lumen of the aneurysmal vessel demonstrates increased attenuation due to contrast enhancement,
whereas the other part of the lumen shows reduced attenuation due to the mural thrombus.
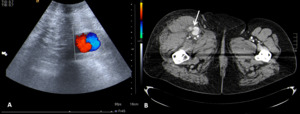
Fig. 11: Femoral artery pseudoaneurism - Ultrasound of the inguinal region (A) showing the characteristic yin-yang sign in color Doppler. Axial (B) contrast-enhanced abdominal CT image proving the pseudoaneurism.
Hematomas can form inside the IC and manifest with pain and edema,
due to compression of the adjacent normal structures.
Causes: trauma,
surgical procedures,
warfarin therapy,
catheter placement or neoplasia.
At CT,
the hematomas usually appear as hyperattenuating masses in IC (attenuation greater than 30 HU).
On ultrasound (figure 12) and MRI,
hematomas may have variable appearance[2].
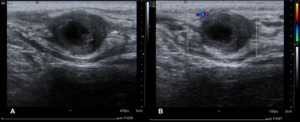
Fig. 12: Ultrasound images (A and B) of the inguinal canal showing a hematoma after local trauma.
D) Tumors
Lipoma is a benign mesenchymal tumor,
composed of mature adipocytes and is the most the most common soft tissue tumor.
On imaging studies,
lipomas are usually discrete,
encapsulated,
homogeneous fatty masses.
The CT and MR images of patients with these lesions are usually sufficiently characteristic to suggest their lipomatous nature and often allow a specific diagnosis[9].
E) Rare conditions
During the development of the embryonic breast,
the ectodermal tissue forms a ridge on the ventral surface,
extending from the axilla towards the midline of the groin.
This ridge is called the mammary ridge or milk line (Figure 13 C).
In normal mammary development,
the mammary ridge recedes,
leaving only bilateral breast tissue at the fourth intercostal space.
When there is a failure of involution of any portion of the embryonic mammary folds,
supernumerary mammary tissue may appear in one of these locations[10].
Ultrasound can be used to differentiate accessory breast tissue from lymphadenopathies lipomas,
sebaceous cysts,
and other masses[11].
In this case (Figure 13 A and B),
the ectopic breast tissue has found incidentally during the abdominal CT scan.
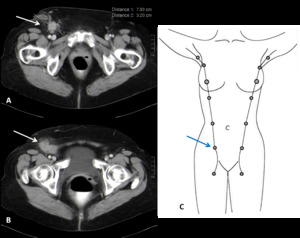
Fig. 13: Axial contrast-enhanced pelvic CT images (A and B) showing a mass occupying the right inguinal region in a 65-year-old woman. A biopsy of this lesion was performed and the histopathological analysis revealed the diagnosis of ectopic breast tissue. C) Illustration of mammary ridge or milk line.
A Nuck cyst is a rare entity that occurs in females when the Nuck canal fails to obliterate.
It presents as a mobile and generally painless,
irreducible inguinal mass that can be transilluminated.
The diagnosis can be easily established with ultrasonography,
which shows cystic mass with a narrow echogenic border (Figure 14 A)[12].
This cyst may have a concomitant inguinal hernia (Nuck hernia),
and in 15% to 20% of cases the ovary enters the canal,
sometimes accompanied by a fallopian tube[13].
In these cases,
early diagnosis is crucial,
because in cases of incarcerated ovaries or strangled loops,
surgical excision is the treatment of choice.
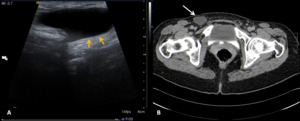
Fig. 14: Ultrasound of the inguinal region (A) showing a cystic mass with a narrow echogenic border (yellow arrows). Axial (B) contrast-enhanced abdominal CT image confirms the presence of a nuck cyst (white arrow).
F) Others
Cryptorchidism is a common congenital anomaly at birth,
occurring in 1.8% to 3.8% of newborns and in up to 30% of premature infants [1,2].
In this condition,
the testicle is not found in the scrotal sac and can be found at any position along its usual line of descent.
Most of the time cryptorchidism is unilateral,
and the testis is located in the inguinal region.
Cryptorchidism should be promptly recognized because it can lead to complications such as torsion of the undescended testis,
infertility,
and malignancy.
Ultrasound (Figure 15 A and B) usually allows the identification of this condition,
but the echogenicity of the undescended testis may vary from hypoechoic to homogeneously hyperechoic[2].
At CT (Figure 15 C and D),
the testes are isoattenuating to soft tissue and show contrast enhancement[2].
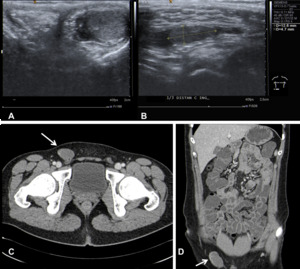
Fig. 15: Ultrasound images (A and B) showing the empty right scrotal sac (A) with a homolateral groin mass (B) corresponding to the undescended testis; Axial (C) and Coronal (D) contrast-enhanced CT enterography images show the undescended testis in the right inguinal canal (white arrows).
Malignant tumors affecting the Inguinal Canal
Liposarcomas are malignant tumors of fatty tissue.
Well-differentiated liposarcomas also resemble lipomas,
although they tend to be larger,
are often traversed by dense bands of collagen,
have gelatinous areas,
and have adipocytes that show more significant variation in size than an ordinary lipoma[9].
CT findings favoring a liposarcoma over a lipoma include inhomogeneous attenuation,
with evidence of significant amounts of soft-tissue within the fatty mass,
poor definition of adjacent structures or the presence of calcifications (figure 16).
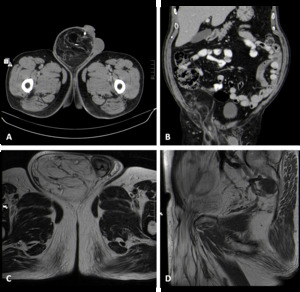
Fig. 16: Axial (A) and Coronal (B) contrast-enhanced abdominal CT images and T2 Axial (C) and T1 Sagittal (D) MR images showing a massive liposarcoma, protruding into the right inguinal canal.
Lymphoma is a neoplasm originating from lymphocytes or lymphoblasts that may be restricted to the lymphatic system or may arise as an extranodal disease.
Lymphomas may have variable aggressiveness and result in a diverse imaging appearance (Figure 17).
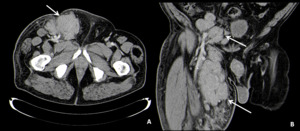
Fig. 17: Axial (A) and Coronal (B) contrast-enhanced abdominal CT images showing IC and thigh involvement in a patient with a non-Hodgkin lymphoma (Follicular lymphoma).
- Metastatic Lymphadenophathy
IC can be a site where malignant neoplasms metastasize,
which can occur by divergent pathways,
such as the hematogenic pathway,
through lymphatic drainage,
or by local invasion of adjacent structures[1].
Metastatic lymph nodes are usually enlarged and on ultrasound,
they arise round or irregular,
heterogeneous or hypoechoic,
with variable vascular flow. A normal echogenic hilum is usually not apparent[1,14].
These increased nodes may also coalesce,
forming a conglomerate,
perceived as a mass in the groin area.
CT (Figure 18) and MR imaging have a complementary role in evaluation of the IC and aid in assessment of disease extent.
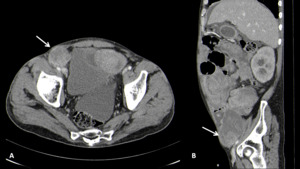
Fig. 18: Axial (A) and Sagittal (B) contrast-enhanced abdominal CT images showing metastatic lymphadenophathy in a patient with a testicular cancer.
