The purpose of radiological imaging in patients with suspected or known cholangiocarcinoma (CCA) is tumour detection,
to establish the presence or abscene of satellite nodules or distant metastases,
lesion characterization and assessment of resectability (tumour’s relationship to the hepatic veins,
inferior vena cava,
the hepatic inflow pedicles and the biliary tree.4-7 Different imaging modalities are implemented complementary in the diagnostic work-up.
Non-invasive imaging should be performed prior to invasive biliary procedures in order to avoid false positive results,
including tumor markers such as carcinoembryonic antigen (CEA),
CA 19-9,
and alpha fetoprotein (AFP).4,5,6
For assessment of intraparenchymal tumor extension and evaluation of biliary and vascular invasion MRI including MRCP and multi-detector,
contrast-enhanced helical CT are the primarily used imaging modalities.4,5 Magnetic resonance imaging (MRI) with magnetic resonance cholangiopancreatography (MRCP) after 3 to 6 hours of fasting,
is probably the best modality to image the biliary tree,
identify mass forming tumours,
ductal or vascular invasion,
and strictures.
It is also preferred by many because it does not require iodinated contrast and does not carry the radiation exposure risk of computed tomography (CT).5,6
Imaging of intrahepatic cholangiocarcinoma (iCCA)
Intrahepatic cholangiocarcinomas can originate from either small intrahepatic ductules (peripheral cholangiocarcinomas) or large intrahepatic ducts proximal to the bifurcation of the right and left hepatic ducts.1
The imaging features of iCCA are dependent on their size and proportion of fibrosis,
necrosis and mucin content.7 Based on macroscopic growth patterns,
iCCA can be divided into mass-forming,
periductal-infiltrating,
intraductal,
and undefined subtypes.3
Ultrasound
Intrahepatic cholangiocarcinoma has variable echogenicity on sonography but tends to be hyperechoic8 and simulate other masses9.
The internal architecture of the tumour is usually homogeneous,
but it can be heterogeneous,
depending on the amount of fibrous tissue,
mucin and calcification.
With contrast enhanced ultrasound,
iCCA may show washout and mimic HCC9 and therefore is not recommended as the sole imaging technique for conclusive diagnosis of HCC10.
CT
On CT,
intrahepatic cholangiocarcinomas can be well defined or infiltrative,
and they lack the fibrous capsules found in HCC.8-10 iCCA are typically hypo- or iso-attenuating relative to normal hepatic parenchyma on unenhanced CT with most remaining hypoattenuating during the arterial and portal venous phases with enhancement only in the delayed phase.
These findings reflect their hypovascular desmoplastic composition.11,12 The periphery of the malignant mass,
in which active tumour growth is found,
enhances rapidly after contrast enhancement and becomes isodense or hypodense during the portal phase.13 Fibrous tissue,
in the central area of the tumor,
does not enhance during the early phase but becomes hyperdense during the delayed phase to 20 minutes later.13,14 The central portion of the tumor remains hypodense,
however,
with necrotic or mucin-producing tumors.
The degree of enhancement varies among tumors and some small mass-forming intrahepatic CCA are arterially enhancing,
mimicking HCC.
The use of delayed phase increases diagnostic confidence in nearly half of the cases.15
MRI
The MR imaging features of iCCA differ according to its pattern of growth.
Mass-forming ICC is irregularly marginated and demonstrates signal intensity depending on the degree of fibrosis,
necrosis,
hemorrhage and mucin within the tumor.13 iCCA is typically hypo to isointense on T1-weighted (T1W) and variably hyperintense on T2-weighted (T2W) imaging.
Following the intravenous administration of gadolinium chelates,
CCA typically show minimal or heterogeneous enhancement at the tumor periphery on early images,
with progressive central enhancement on subsequent delayed image16 owing to the fibrous composition.17
Imaging of perihilar cholangiocarcinoma.
(pCCA)
pCCAs develop anywhere from the second-order biliary ducts to above the site of cystic duct origin.
It has been further classified according to the pattern of involvement of the hepatic ducts with the Bismuth-Corlette classification: Type I lesions involve the common hepatic duct (CHD) immediately below the confluence; type II tumors involve the CHD and extend to the confluence but not beyond; type IIIa masses involve the CHD to the confluence and extend into the main right hepatic duct; type IIIb lesions involve the CHD to the confluence and extend into the main left hepatic duct and type IV tumors involve the CHD and extend past the confluence involving both the right and left hepatic ducts; they can have exophytic (mass-forming) and intraductal growth patterns.3
Ultrasound
The sensitivity and accuracy of ultrasound for diagnosis of extrahepatic CCA is 89% and 80-95% respectively12,19 and is useful in ruling out benign causes of bile duct obstruction18.
Lesions that form masses and invade surrounding liver parenchyma or involve portal vessels can be demonstrated on ultrasound.18
CT
The accuracy of CCA diagnosis with MDCT is markedly improved when images are obtained with thin collimation in the arterial,
portal venous and delayed phases.
Perihilar CCA often appears as a heterogeneous,
hypervascular lesion in the delayed-phase images.20 Multidetector CT has 78.6%-92.3% accuracy for diagnosis of extrahepatic CCA13 but has strong tendency to underestimate the longitudinal extension of the tumor20.
The accuracy for detection of portal vein and arterial involvement has been reported to be as high as 87% and 93% respectively.21 However,
its sensitivity in the detection of regional lymphadenopathy is only 54% and CT tends to underestimate the extent of proximal tumour.22
CT cholangiography is superior to conventional CT or US and equal to ERCP for diagnosis of pCCA.21 A potential limitation of CT cholangiography is the dependence on the secretory function of the biliary system that may be compromised in patients with high-grade obstruction or significantly elevated bilirubin levels.11
MRI/MRCP
When viewing CCA on MRI,
the lesion often appears hypointense compared with the liver parenchyma on T1-weighted images and hyperintense on T2-weighted images.23 MRI with MRCP is the imaging technique of choice in many centers secondary to its excellent soft tissue contrast that is particularly useful for evaluation of infiltrating ductal tumorus.23 MRI with MRCP has an accuracy of 66% for detection of lymph node metastases24,
78% sensitivity and 91% specificity for portal vein invasion25 and 58-73% sensitivity and 93% specificity for hepatic arterial invasion.26
Imaging of distal cholangiocarcinoma.
(dCCA)
dCCA develops anywhere between the cystic duct origin and the ampulla of Vater (without its involvement).3
Distinct features and imaging characteristics of this type are not well known as these are frequently clubbed with pCCA and referred to as extrahepatic CCA.18
Ultrasound is useful to demonstrate the obstruction level,
CT and MRI with MRCP may demonstrate thickening and/or stricturing of bile duct with proximal duct dilatation and sometimes a mass.27
Four patients aged 63-87 years (M:F=4:0) presented with weight loss,
malaise,
abdominal discomfort and jaundice,
underwent clinical examination followed by CT imaging and pathologic diagnosis:
• A 63 year old male patient was transferred to our hospital for further evaluation,
when suspicion on cholangiocarcinoma was made after he presented with abdominal pain and painless jaundice.
Biliary stent was placed prior to his transfer.
MSCT showed soft tissue mass surrounding common bile duct,
expanding in left hepatic duct with consequent dilatation of peripheral bile ducts,
more prominent in left liver lobe.
The mass infiltrates pancreatic head,
is in contact with gallbladder and descending part of duodenum.
PHD was taken,
sample was positive on malignant cells and diagnosis of cholangiocarcinoma was made.
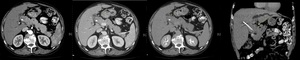
Fig. 1: Perihilar cholangiocarcinoma. (a,b,c,d) Contrast enhanced axial arterial, venous, delayed phase and coronal arterial phase CT scans show common bile duct surrounded by soft tissue mass and dilatation of peripheral bile ducts. Biliary stent in common bile duct is also visible.
References: Department of Radiology, Clinical Hospital Merkur/Croatia 2018
• A 77 year old male patient presented in ER with upper right abdominal pain and progressive weight loss in 3 months period.
Physical exam showed enlarged liver and ultrasound revealed multiple homogeneous hypoechoic masses in right liver lobe.
MSCT was indicated and revealed big,
necrotizing hypoattenuating mass in right liver lobe,
pushing on ventral edge of right kidney with peripheral enhancement in the delayed phase.
Partial ductal dilatation could not be excluded.
Biopsy and PHD analysis were performed and cholangiocarcinoma was verified.

Fig. 2: Mass forming cholangiocarcinoma. (a,b,c) Contrast enhanced axial arterial, venous and delayed phase CT scans show an irregular hypoattenuating lesion with heterogenous peripheral enhancement.
References: Department of Radiology, Clinical Hospital Merkur/Croatia 2018
• A 68 years old male patient presented with high erythrocyte sedimentation rate on routine laboratory testing at general practice couple of weeks prior coming to hospital.
Elective ultrasound revealed expansive mass in right liver lobe near medial contour,
hyperechoic abnormalities of pancreatic head and body parenchyma,
perihilar and periportal lymph nodes without intra- and extra- ductal dilatation.
MSCT was indicated and revealed hypoattenuating,
inhomogenous,
ill defined mass with peripheral enhancement and conglomerate of hypodense necrotic peripancreatic,
periportal,
perihepatal and hilar lymph.
Findings were indicative of cholangiocarcinoma which was verified histopathologically.
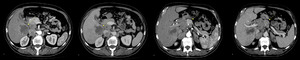
Fig. 3: Mass forming cholangiocarcinoma. (a,b) Contrast enhanced arterial and venous phase CT scans show irregular hypoattenuating lesion in segment V with minimal peripheral enhancement of the lesion.
(c,d) Contrast enhanced CT scans obtained 2cm higher than a and b in arterial and venous phase show multiple enlarged limph nodes unseparable from pancreatic head and portal vein with soft tissue mass in both adrenal glands (highly suggestive of metastatic process).
References: Department of Radiology, Clinical Hospital Merkur/Croatia 2018
• A 87 year old male patient presented with painless jaundice and weight loss.
Elective ultrasound showed dilatation of intra- and extra- hepatic bile ducts with focal lesion in right liver lobe.
MSCT showed fatty liver,
tumoral involvement of the common bile duct lumen at the cystic duct junction with consequent proximal dilatation of intrahepatic ducts and liver lesion at the border of segment VIII and IVa (characteristics of metastasis).
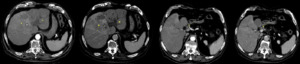
Fig. 4: Perihilar cholangiocarcinoma. (a,b) Contrast enhanced axial arterial and venous phase CT scans show hypoattenuating intrahepatic lesion with peripheral enhancement and dilatation of intrahepatic ducts.
(c,d) Contrast enhanced axial arterial and venous phase CT scans obtained 1 cm lower than a and b show common bile duct with tumor infiltration with post contrast enhancement and total obliteration of the distal lumen.
References: Department of Radiology, Clinical Hospital Merkur/Croatia 2018

Fig. 5: Contrast enhanced coronal venous phase CT scan shows common bile duct dilatation with tumor infiltration (arrow).
References: Department of Radiology, Clinical Hospital Merkur/Croatia 2018
