The ultrasound study can be optimized considering the patient's position,
the probe type,
the amount of gel,
the ultrasound parameters,
and the knowledge of ultrasound HN anatomy.
1.
Patient Positioning
The examiner should be sufficiently comfortable to maintain his position during the examination.
In the supine position,
the head of the patient is in mild extension.
The base of the neck should not be covered.
A thin pillow should be at hand to place underneath the patient’s shoulders if the examination requires hyperextension of the neck.
If the patient cannot lie down,
the examination can be done in the sitting position.
2.
Ultrasound settings and Probe type
Choosing suitable preset settings will limit the amount of control adjustment required during the patient examination.
The parameters typically include frequency,
gain,
depth of the focal zone,
zoom and depth of the field. The ability to manually adjust specific parameters enables individual optimization Fig. 1 .
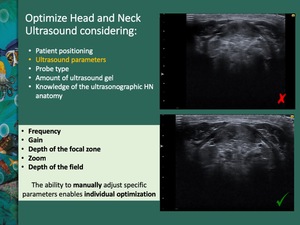
Fig. 1: Optimization of ultrasound parameters: frequency, gain, depth of the focal zone, zoom and depth of the field. The ability to manually adjust specific parameters enables individual optimization.
References: Department of Radiology, IPO Porto, Porto, 2018
High-frequency linear transducers (7,5 to 12MHz or greater) are indicated for HN ultrasound imaging Fig. 2 .
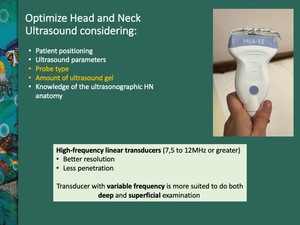
Fig. 2: Probe type - high-frequency linear transducers are the indicated for HN ultrasound imaging
References: Department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018
With a higher frequency,
there is a better resolution but with less penetration.
Therefore,
a transducer with variable frequency is more suited to perform both deep and superficial examination of head and neck structures.
With thin necks,
frequencies of 10 to 12MHz provide clear images of the thyroid; a depth of 45mm is enough to identify vertebral bodies in the lower part of the image.
The oropharynx and the tongue require the increase of depth to 60-70mm.
Larger necks or deeper lesions are better evaluated with lower frequencies,
to achieve better tissue penetration.
|
HIGHER FREQUENCIES
|
LOWER FREQUENCIES
|
|
Thyroid isthmus
|
Parathyroid glands
|
|
Superficial lymph nodes
|
Deep muscles and lymph nodes
|
|
|
Deep parotid
|
|
|
Tongue
|
Gain refers to the overall brightness of the image.
Gain can be adjusted throughout the examination.
It can help to define areas of pathology in relation to surrounding tissues.
Depth can also be changed during the exam,
depending on depth of the object of greatest interest.
Adjusting focal zone is useful when examining deep and superficial objects in the same patient.
Any anatomical region should be examined in two perpendicular planes.
Doppler ultrasound is an important examination adjunct.
A generous amount of ultrasound gel should be applied to the patient’s neck for ultrasound transduction Fig. 2 .
3.
Head and Neck Ultrasound - Step by Step
Once the orientation of the probe is correct,
a personal algorithm should be followed in order to avoid forgetting anatomical structures.
We propose some HN sonographic steps Fig. 3 :
- Submental
- Submandibular
- Parotid and buccal
- Deep cervical chain
- Transverse cervical
- Posterior triangle
- Anterior cervical,
including thyroid.
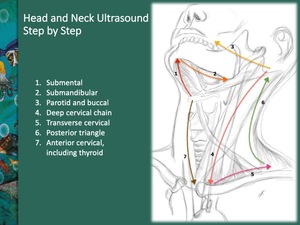
Fig. 3: Ultrasonographic systematic approach in seven steps: 1.submental; 2.submandibular; 3.parotid and buccal; 4.deep cervical chain; 5.transverse cervical; 6.posterior triangle; and 7.anterior cervical, including thyroid
References: Catarina Baraças, ULS Matosinhos, PT 2018
Submental Region
Step 1: Run the probe at the midline,
from chin to hyoid.
Mylohyoid and hyoglossus muscles are the keys.
Fig. 3: Ultrasonographic systematic approach in seven steps: 1.submental; 2.submandibular; 3.parotid and buccal; 4.deep cervical chain; 5.transverse cervical; 6.posterior triangle; and 7.anterior cervical, including thyroid
References: Catarina Baraças, ULS Matosinhos, PT 2018
The submental triangle can be defined on ultrasound Fig. 4 .
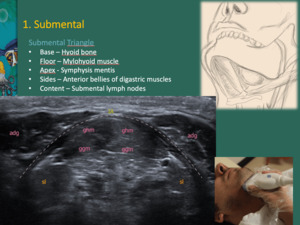
Fig. 4: Submental triangle - Hyoid bone is at the base of the triangle; mylohyoid muscle (dashed line) is on the floor and the symphysis mentis represents the apex. The anterior belly of the digastric muscle (adg) covers both sides of the triangle. They can be assessed in transverse section to the hyoid. Submental lymph nodes (IA) represent the triangle content.
The root of the tongue is composed by genioglossus (ggm) and geniohyoid muscles (ghm). Both muscles, in conjunct with the hyoglossus muscle (hgm), represent the major extrinsic muscles of the tongue.
Sl – sublingual salivary glands
References: Department of Radiology, IPO Porto, Porto, 2018
The root of the tongue is composed by genioglossus and geniohyoid muscles (genial muscles).
Both muscles,
in conjunct with the hyoglossus muscle,
represent the major extrinsic muscles of the tongue Fig. 4 Fig. 5 .
Two mylohyoid muscles run between the medial aspect of the mandibular bodies to form the floor of the mouth.
They are attached to the mandibular body,
immediately inferior to genial muscles.
Anteriorly they are thinner,
and thus,
hardly seen.
Posteriorly they have free thick borders.
Hyoglossus muscle depresses the tongue.
Mylohyoid and hyoglossus muscles can be differentiated asking the patient to move the tongue from side to side,
while scanning in the coronal plane.
Hyoglossus muscle contracts while mylohyoid muscle is immobile Fig. 5 .
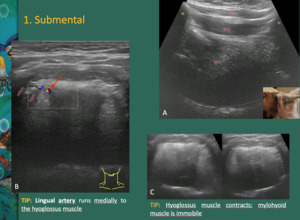
Fig. 5: A - The root of the tongue is composed by genioglossus (ggm) and geniohyoid muscles (ghm).
Dashed line: dorsal surface of the tongue; M – mandible; H – hyoid bone; adg – anterior belly of the digastric muscle
B - Lingual artery is a landmark. It runs medially to the hyoglossus muscle (hgm).
C - Mylohyoid and hyoglossus muscles can be differentiated asking the patient to move the tongue from side to side, while scanning in the coronal plane. Hyoglossus muscle contracts while mylohyoid muscle is immobile.
References: Department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018
The lingual artery is a landmark.
It runs medially to the hyoglossus muscle.
The submandibular duct runs laterally to the hyoglossus muscle.
If dilated,
it can be easily identified.
Color Doppler helps to distinguish the submandibular duct from the lingual vein Fig. 5 Fig. 6 .
Both submandibular duct and sublingual gland are between the hyoglossus and the mylohyoid muscles.
They are superolateral to the lingual artery,
which is medial to the hyoglossus muscle.
Fig. 7
The sublingual gland is a hyperechoic structure,
lateral to the hyoglossus muscle.
Anteriorly it reaches the symphysis mentis and posteriorly it touches the deep surface of the submandibular gland.
Sometimes an accessory duct joins the submandibular duct.
A single sublingual-submandibular complex is also possible.
The mylohyoid muscle is the key to determinate the origin of a lesion.
It separates the sublingual space (deep to mylohyoid muscle) from the submandibular space (superficial).
Posteriorly,
the free border of the mylohyoid muscle enables the communication between these two spaces and the inferior parapharyngeal space.
The submandibular duct extends anteriorly from the submandibular space and deviates medially into the sublingual space through the free posterior border of the mylohyoid muscle.
Fig. 7
Submandibular Region
Step 2: Run the ultrasound probe from the chin to mandible angle.
Follow mylohyoid muscle.
Fig. 3: Ultrasonographic systematic approach in seven steps: 1.submental; 2.submandibular; 3.parotid and buccal; 4.deep cervical chain; 5.transverse cervical; 6.posterior triangle; and 7.anterior cervical, including thyroid
References: Catarina Baraças, ULS Matosinhos, PT 2018
The submandibular gland is sitting on the digastric and mylohyoid muscles,
when the probe is in a transverse plane.
The anterior belly of the digastric muscle is in the same plane as the submandibular gland,
so it can be better identified in parasagittal planes of the submandibular gland.
Fig. 6
The anterior belly of the digastric muscle arises anteriorly and the tendinous part of the posterior belly arises posteriorly to the body of the gland.
The posterior belly is harder to see because it is less muscular; it can be seen running posteriorly up to the hyoid bone.
Posteriorly,
the mylohyoid muscle indents the submandibular gland with its free border.
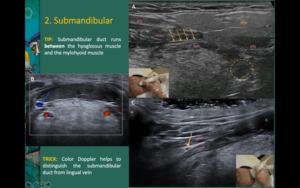
Fig. 6: A - The submandibular gland is sitting on the digastric and mylohyoid muscles.
A, C - The submandibular duct (yellow arrows) runs laterally to the hyoglossus muscle (hgm).
B - Color Doppler helps to distinguish the submandibular duct from lingual vein (blue arrow).
adg - anterior belly of the digastric muscle; pdg - posterior belly of the digastric muscle; mhm - mylohyoid muscle; Dashed circle: tonsil; M – mandible; H – hyoid bone
References: Department of Radiology, Hospital Pedro Hispano, ULS Matosinhos, Portugal 2018; Department of Radiology, IPO Porto, Porto, 2018
Anteriorly to the gland,
a fatty space can be identified,
with lymph nodes.
There are always two venous landmarks in this region: the facial vein and the anterior division of the retromandibular vein (RMV).
The facial vein runs anteriorly and superiorly to the gland,
and the RMV runs posteriorly to the gland and joins the facial vein to drain into the internal jugular vein (IJV).
The displacement of the RMV helps to determine if a lesion comes from the submandibular or the parotid gland.
Fig. 8
The facial artery has a tortuous course.
It passes obliquely up above both the posterior belly of the digastric and the stylohyoid muscles (from medial to lateral) and it arches to enter a groove on the posterior surface of the submandibular gland; it then curves upward the inferior border of the mandible.
Parotid and Buccal
Step 3: Run the ultrasound probe from the external auditory meatus to the angle of the mouth.
Follow the parotid duct.
Fig. 3: Ultrasonographic systematic approach in seven steps: 1.submental; 2.submandibular; 3.parotid and buccal; 4.deep cervical chain; 5.transverse cervical; 6.posterior triangle; and 7.anterior cervical, including thyroid
References: Catarina Baraças, ULS Matosinhos, PT 2018
The RMV descends in the substance of the parotid,
is superficial to the external carotid artery and underneath the facial nerve.
Thus,
the RMV is an important reference to the facial nerve.
Fig. 8
The RMV helps to differentiate between superficial and deep parotid lobes.
It is important for the choice of surgical procedure,
in order to decrease the risk of damaging the facial nerve.
A line through the axis of the ramus of the mandible can also divide parotid lobes.
The deep lobe is not accurately assessed with ultrasound.
If the ultrasonographer found a pathology,
it should be studied with cross-sectional imaging.
The main parotid duct is identified as an echogenic line within the superficial lobe.
Fig. 8
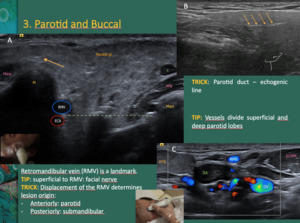
Fig. 8: A -The retromandibular vein (RMV) descends in the substance of the parotid gland, between the ramus of the mandible (M) and the sternocleidomastoid muscle. It is superficial to the external carotid artery (ECA) and beneath the facial nerve. The vessels are an arbitrary reference to divide the parotid gland into superficial and deep lobes.
B - The main parotid duct is identified as an echogenic line (yellow arrows) within the superficial lobe. It runs forward along the lateral side of the masseter muscle (mass), about 1cm/1,5cm below the zygomatic arch, entering the buccal space and piercing the buccinator muscle.
C – The RMV is a landmark. The displacement of the vein helps determining lesion origin; if it displaces anteriorly the lesion will usually be from the parotid; posterior displacement is more likely to be caused by a submandibular lesion
Mast – mastoid; Pdg - Posterior belly of the digastric muscle; IIA – deep cervical lymph node chain; * Intraparotid lymph node; ECCM – sternocleidomastoid muscle; IJV – internal jugular vein
References: Department of Radiology, Hospital Pedro Hispano, ULS Matosinhos, Portugal 2018; Department of Radiology, IPO Porto, Porto, 2018
The masseter muscle is covered posteriorly by the anterior part of the parotid gland.
Accessory lobes of the parotid are identified in this region.
Fig. 9
The buccinator muscle is deep and anterior to the masseter muscle.
Buccinator muscle can be better identified asking the patient to puff their cheeks out Fig. 9 .
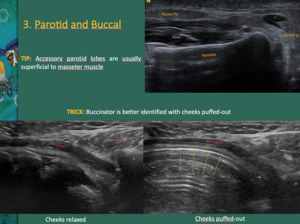
Fig. 9: Accessory lobes (Access PG) of the parotid are identified in this region, superficial to the masseter (mass) muscle.
The buccinator muscle is deep and anterior to the masseter muscle. The buccinator muscle can be better identified asking the patient to puff their cheeks out. The buccal space contains the facial nerve, artery and vein, fat pad (adults have less fat than children) and parotid duct.
*Intraparotid lymph node; Green arrows - buccal mucosal interface
References: Department of Radiology, Hospital Pedro Hispano, ULS Matosinhos, Portugal 2018; Department of Radiology, IPO Porto, Porto, 2018
Deep Cervical Chain
Step 4: Run the ultrasound probe from the angle of the jaw to the supraclavicular fossa.
Follow the IJV.
Fig. 3: Ultrasonographic systematic approach in seven steps: 1.submental; 2.submandibular; 3.parotid and buccal; 4.deep cervical chain; 5.transverse cervical; 6.posterior triangle; and 7.anterior cervical, including thyroid
References: Catarina Baraças, ULS Matosinhos, PT 2018
The hyoid bone divides the upper and mid cervical regions.
The cricoid cartilage divides mid and lower cervical regions.
The posterior belly of the digastric muscle is a reference to separate the parotid gland from the upper cervical region.
It also divides the submandibular triangle anteriorly and the carotid triangle posteriorly. Fig. 3 To identify the posterior belly of the digastric muscle,
the ultrasound probe should be put between the submandibular gland and the mastoid process and then direct it down to the hyoid bone – the probe should be at 45 degrees to the vertical plane of the parotid gland.
The posterior belly of the digastric muscle touches the parotid tail and goes deeply to the sternocleidomastoid muscle.
The RMV is superficial to the posterior belly.
Sliding the probe down the plane of the posterior belly of the digastric muscle,
the deep vessels are seen,
from posterior to anterior: the IJV,
internal carotid artery and external carotid artery.
Color flow can guide the evaluation of this region.
The deep cervical lymph node chain runs along the IJV; thus,
the IJV should be at the middle of the field of view.
Fig. 10
During the transverse scan,
the IJV should be compressed,
in order to detect thrombus.
Inside the carotid sheath,
the vagus nerve is between the common carotid artery (CCA) and the IJV.
It appears as a centrally hypoechoic and peripherally hyperechoic structure.
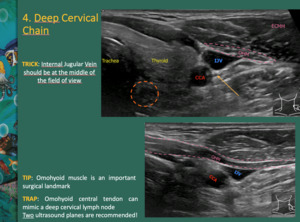
Fig. 10: The deep cervical lymph node chain runs along the internal jugular vein (IJV); thus, the IJV should be at the middle of the field of view.
Inside the carotid sheath, the vagus nerve (yellow arrow) is between the common carotid artery (CCA) and the IJV.
Omohyoid muscle is an important surgical landmark. Usually, the omohyoid muscle crosses the common carotid artery (CCA) at the level of the cricoid cartilage. Thus, omohyoid muscle can split mid from lower cervical chain.
Dashed circle: esophagus; OHM – omohyoid muscle; ECMM – sternocleidomastoid muscle
References: Department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018
Thin necks allow finding the transverse process of the atlas between the mastoid process and the angle of the mandible.
The omohyoid muscle is an important surgical landmark.
The omohyoid muscle has two bellies: the superior and the inferior.
The superior belly runs obliquely from the hyoid body,
crosses anteriorly to the CCA and posteriorly to the sternocleidomastoid muscle.
Usually,
the omohyoid muscle crosses the CCA at the level of the cricoid cartilage,
splitting mid from lower cervical chain.
The central tendon overlies the IJV or is immediately lateral – sometimes it is wrongly called a lymph node.
It is important to do transverse and vertical planes.
The superior belly of the omohyoid muscle subdivides the infrahyoid part of the anterior triangle: carotid and muscular triangles.
The inferior belly runs posteriorly and attaches to the clavicle.
The inferior (or posterior) belly divides the posterior triangle: occipital (upper) and subclavian (inferior) triangles.
Supra-omohyoid lymph node dissection is typical with cervical tumor resection.
The omohyoid muscle is an important reference in neck surgery.
The esophagus is identified medially to the CCA,
usually on the left of the trachea.
If hard to see,
ask the patient to swallow.
Fig. 10
Run the probe until finding the junction of the common carotid and subclavian arteries.
Angle the probe inferiorly to see the subclavian artery behind the clavicle.
Cervical Transverse
Step 5: Run the probe from the sternoclavicular joint to the acromioclavicular joint.
Screen along the sternocleidomastoid and trapezius muscle.
Fig. 3: Ultrasonographic systematic approach in seven steps: 1.submental; 2.submandibular; 3.parotid and buccal; 4.deep cervical chain; 5.transverse cervical; 6.posterior triangle; and 7.anterior cervical, including thyroid
References: Catarina Baraças, ULS Matosinhos, PT 2018
The landmark of the root of the neck is the scalenus anterior muscle.
Fig. 11
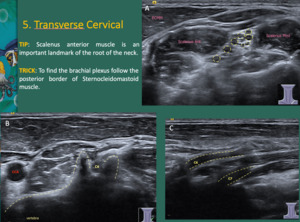
Fig. 11: A - The landmark of the root of the neck is the scalenus anterior muscle. It runs from the transverse processes of the cervical spine, passes behind the IJV and the clavicle, and attaches to the first rib. It also runs between subclavian artery, posteriorly, and subclavian vein anteriorly.
Between scalenus anterior and scalenus medius muscles, the brachial plexus (root and trunks) appear as rounded hypoechoic structures (dashed yellow circles). A tip to find the brachial plexus is to follow the posterior border of the sternocleidomastoid muscle (ECMM).
B- A transverse plane at the lower neck allows seeing C6 nerve root (C6).
C - Longitudinal plane allows seeing C6 and C7.
References: Department of Radiology, IPO Porto, Porto, 2018
The transverse plane at the lower neck allows seeing C6 nerve root.
The longitudinal plane allows seeing C6 and C7.
The brachial plexus (root and trunks) is seen between the scalenus anterior and scalenus medius muscles,
as a cluster of rounded hypoechoic structures.
Angling the probe inferiorly allows for the apex of the lung to show up with reverberation artifact.
Posterior Triangle
Step 6: Run the probe from the acromioclavicular joint upward to the mastoid.
Follow the anterior border of the trapezius muscle.
Fig. 3: Ultrasonographic systematic approach in seven steps: 1.submental; 2.submandibular; 3.parotid and buccal; 4.deep cervical chain; 5.transverse cervical; 6.posterior triangle; and 7.anterior cervical, including thyroid
References: Catarina Baraças, ULS Matosinhos, PT 2018
Inferiorly,
parallel to the clavicle,
the transverse cervical artery and vein are seen arising from the thyrocervical trunk and IJV,
respectively.
The spinal accessory nerve and the lymph node chain runs from between the mastoid process and the angle of the mandible to the outer third of the clavicle.
Running the posterior triangle on a transverse plane shows the transverse processes of the vertebrae as echogenic structures with posterior acoustic shadowing and they should not be mistaken with calcified lymph nodes.
Fig. 12
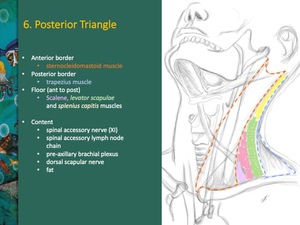
Fig. 12: Posterior triangle is very superficial. It is a fat filled superficial structure.
The posterior border of the sternocleidomastoid muscle represents the anterior border of the triangle; the anterior border of the trapezius muscle is responsible for the posterior border of the triangle. From anterior to posterior, the floor is composed by scalene, levator scapulae and splenius capitis muscles.
The posterior triangle contains the spinal accessory nerve (XI), spinal accessory lymph node chain, pre-axillary brachial plexus, dorsal scapular nerve and fat.
References: Catarina Baraças, ULS Matosinhos, PT 2018
Cervical Anterior
Step 7: Run the probe at the midline from the hyoid bone to the sternal notch.
Screen larynx and thyroid.
Fig. 3: Ultrasonographic systematic approach in seven steps: 1.submental; 2.submandibular; 3.parotid and buccal; 4.deep cervical chain; 5.transverse cervical; 6.posterior triangle; and 7.anterior cervical, including thyroid
References: Catarina Baraças, ULS Matosinhos, PT 2018
The strap muscles are thin muscles covering the midline.
Detailed anatomy is important to localize thyroglossal duct cysts and anterior cervical lymph nodes.
Fig. 13
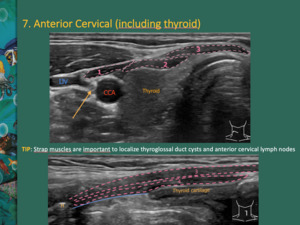
Fig. 13: The strap muscles are thin muscles covering the midline. They help to localize thyroglossal duct cysts and anterior cervical lymph nodes.
1 - omohyoid muscle (superior belly); 2 – sternothyroid muscle; 3 – sternohyoid muscle; 4 – thyrohyoid muscle; arrow - vagus nerve; blue line: thyrohyoid membrane; IJV - internal jugular vein; CCA - common carotid artery
References: Department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018
The sonographer should be able to recognize some laryngeal landmarks,
such as epiglottis and pre-epiglottic space.
They are best seen in sagittal sections Fig. 14 .
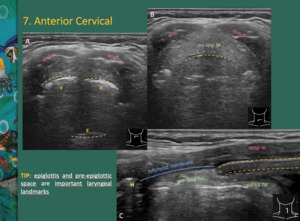
Fig. 14: A, B - Laryngeal landmarks: epiglottis (E) and pre-epiglottic space. V - vallecullae
C- Pre epigl fat: pre-epiglottic fat; paragl fat: paraglottic fat; strap m: strap muscles; H – hyoid bone
References: department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018
False and true vocal cords can be recognized in axial and parasagittal sections.
Fig. 15
The cricoid cartilage is a good midline anatomical reference.
It usually lies inferiorly to the thyroid isthmus.
It is a wide cartilaginous structure which differs from tracheal rings in thickness.
Fig. 15
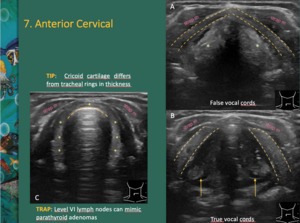
Fig. 15: A, B - False and true vocal cords can be recognized in axial and parasagittal sections. Green * - paraglottic fat; yellow dashed lines: thyroid cartilage; yellow arrow – arytenoids
C – Cricoid cartilage differs from tracheal rings in thickness. Dashed yellow lines: air-mucosal interface; yellow * - cricoid cartilage.
Strap m – strap muscles
References: department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018
Ultrasound can help to perform a percutaneous tracheostomy (preferable between the first and the second tracheal rings),
especially in the obese or edematous necks,
patients with large thyroid isthmus or venous anomalies.
Level VI lymph nodes can be mistaken for parathyroid adenomas.
The thymus can be seen through the suprasternal notch.
Normal gland contains scattered echogenic foci.




 is on the floor and the symphysis mentis represents the apex. The anterior belly of the digastric muscle (adg) covers both sides of the triangle. They can be assessed in transverse section to the hyoid. Submental lymph nodes (IA) represent the triangle content.
The root of the tongue is composed by genioglossus (ggm) and geniohyoid muscles (ghm). Both muscles, in conjunct with the hyoglossus muscle (hgm), represent the major extrinsic muscles of the tongue.
Sl – sublingual salivary glands References: Department of Radiology, IPO Porto, Porto, 2018")
 and geniohyoid muscles (ghm).
Dashed line: dorsal surface of the tongue; M – mandible; H – hyoid bone; adg – anterior belly of the digastric muscle
B - Lingual artery is a landmark. It runs medially to the hyoglossus muscle (hgm).
C - Mylohyoid and hyoglossus muscles can be differentiated asking the patient to move the tongue from side to side, while scanning in the coronal plane. Hyoglossus muscle contracts while mylohyoid muscle is immobile.
References: Department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018")
 runs laterally to the hyoglossus muscle (hgm).
B - Color Doppler helps to distinguish the submandibular duct from lingual vein (blue arrow).
adg - anterior belly of the digastric muscle; pdg - posterior belly of the digastric muscle; mhm - mylohyoid muscle; Dashed circle: tonsil; M – mandible; H – hyoid bone References: Department of Radiology, Hospital Pedro Hispano, ULS Matosinhos, Portugal 2018; Department of Radiology, IPO Porto, Porto, 2018")

 descends in the substance of the parotid gland, between the ramus of the mandible (M) and the sternocleidomastoid muscle. It is superficial to the external carotid artery (ECA) and beneath the facial nerve. The vessels are an arbitrary reference to divide the parotid gland into superficial and deep lobes.
B - The main parotid duct is identified as an echogenic line (yellow arrows) within the superficial lobe. It runs forward along the lateral side of the masseter muscle (mass), about 1cm/1,5cm below the zygomatic arch, entering the buccal space and piercing the buccinator muscle.
C – The RMV is a landmark. The displacement of the vein helps determining lesion origin; if it displaces anteriorly the lesion will usually be from the parotid; posterior displacement is more likely to be caused by a submandibular lesion
Mast – mastoid; Pdg - Posterior belly of the digastric muscle; IIA – deep cervical lymph node chain; * Intraparotid lymph node; ECCM – sternocleidomastoid muscle; IJV – internal jugular vein References: Department of Radiology, Hospital Pedro Hispano, ULS Matosinhos, Portugal 2018; Department of Radiology, IPO Porto, Porto, 2018")
 of the parotid are identified in this region, superficial to the masseter (mass) muscle.
The buccinator muscle is deep and anterior to the masseter muscle. The buccinator muscle can be better identified asking the patient to puff their cheeks out. The buccal space contains the facial nerve, artery and vein, fat pad (adults have less fat than children) and parotid duct.
*Intraparotid lymph node; Green arrows - buccal mucosal interface References: Department of Radiology, Hospital Pedro Hispano, ULS Matosinhos, Portugal 2018; Department of Radiology, IPO Porto, Porto, 2018")
; thus, the IJV should be at the middle of the field of view.
Inside the carotid sheath, the vagus nerve (yellow arrow) is between the common carotid artery (CCA) and the IJV.
Omohyoid muscle is an important surgical landmark. Usually, the omohyoid muscle crosses the common carotid artery (CCA) at the level of the cricoid cartilage. Thus, omohyoid muscle can split mid from lower cervical chain.
Dashed circle: esophagus; OHM – omohyoid muscle; ECMM – sternocleidomastoid muscle References: Department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018")
 appear as rounded hypoechoic structures (dashed yellow circles). A tip to find the brachial plexus is to follow the posterior border of the sternocleidomastoid muscle (ECMM).
B- A transverse plane at the lower neck allows seeing C6 nerve root (C6).
C - Longitudinal plane allows seeing C6 and C7.
References: Department of Radiology, IPO Porto, Porto, 2018")
, spinal accessory lymph node chain, pre-axillary brachial plexus, dorsal scapular nerve and fat.
References: Catarina Baraças, ULS Matosinhos, PT 2018")
; 2 – sternothyroid muscle; 3 – sternohyoid muscle; 4 – thyrohyoid muscle; arrow - vagus nerve; blue line: thyrohyoid membrane; IJV - internal jugular vein; CCA - common carotid artery References: Department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018")
 and pre-epiglottic space. V - vallecullae
C- Pre epigl fat: pre-epiglottic fat; paragl fat: paraglottic fat; strap m: strap muscles; H – hyoid bone References: department of Radiology, Hospital Pedro Hispano,ULS Matosinhos, Portugal 2018")
