ECR 2019 / C-2920
Lateral knee pain: A comprehensive sonographic spectrum of pathologies and guided interventions
Congress:
ECR 2019
Poster Number:
C-2920
Type:
Educational Exhibit
Keywords:
Trauma, Inflammation, Diagnostic procedure, Ultrasound, Musculoskeletal system, Interventional non-vascular
Authors:
P. jain1, D. K. Singh2, N. KUMAR1, B. K. Nayak1, A. Katyan1, S. Suman3, S. Tomar3, S. B. Grover3; 1New Delhi , Delhi/IN, 2delhi/IN, 3New Delhi/IN
DOI:
10.26044/ecr2019/C-2920

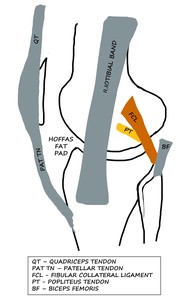
Fig. 1:
LK: Schematic diagram showing the anterolateral and some of the posterolateral...

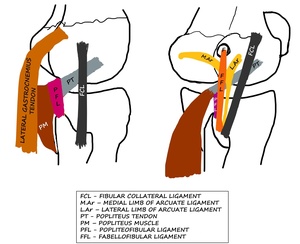
Fig. 2:
LK: Schematic diagram showing the posterolateral corner structures of LK.

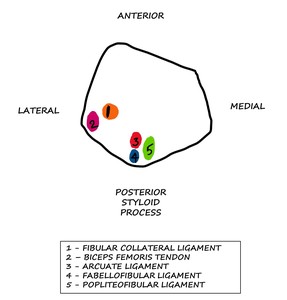
Fig. 3:
LK: Schematic diagram showing the attachments of ligaments and tendons on the...