Emphysematous kidney lesions; include emphysematous pylitis,
emphysematous pylonephrosis (EPN) and perinephric abscess are relatively rare condition.
It results from sever parenchymatous kidney infection by anaerobic gas forming bacteria usually ascending infection.
E-coli is isolated on urine or pus cultures in nearly 70% of the reported cases.
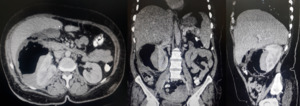
Fig. 2: 53 year-old female diabetic presented by acute kidney injury with high grad fever and hyperglycemia not responding to Usual treatment. CT revealed emphysematous perinephritis.
EPN tends to be common in middle and old age patients ( usually > 50 year-old ) with uncontrolled diabetic (Up to 95% of the EPN cases ) and more common within females ( Few studies reported that female: male ratio is 6:1) .The risk of developing EPN secondary to a urinary tract obstruction is about 25–40%.
and the recurrent ascending infections seem to be the main cause in the female predominance.
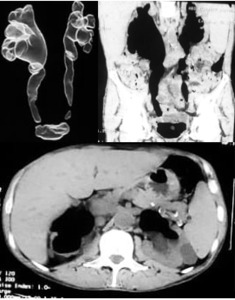
Fig. 4: 62 year -old male patient known case of advanced stage cancer rectum invading both ureters presented with high grad fever and deteriorated renal function. (quoted from Dr. Karim AbdelTawab,MD , IR Ain-Shams university hospitals)
The untreated cases have a high mortality rate.
The septic complications are the main cause of mortality in EPN.
Poor Prognostic factors include:
- The presence of thrombocytopenia.
- Bilateral EPN.
- poor glycaemic control.
Increased mortality rate is associated with :
- Systolic blood pressure less than 90 mmHg.
- Disturbance of consciousness .
- Increased serum creatinine level.
- Treatment with antibiotics alone is associated with a higher risk of mortality compared to either percutaneous drainage (PCD) or nephrectomy.
The mortality depends on the percentage of destruction of the renal parenchyma.
It could be classified into
- Type 1: destruction is more than 30% of the parenchyma with the gas is within the renal parenchyma with a little amount of fluid.
it has a mortality rate of 70%
- Type 2 : destruction is less than 30 % of the parenchyma while gas is confined to the collecting system only with fluid.
It has a mortality rate of 18%.
Huang et al CT classifies the EPN into
- class 1: gas in collecting system only
- class 2: gas in renal parenchyma only (without extrarenal extension)
- class 3: gas in renal parenchyma with extrarenal extension
-
- class 3a: extension of gas or abscess to perinephric space
- class 3b: extension of gas or abscess to pararenal space
- class 4: bilateral emphysematous pyelonephritis or solitary kidney with emphysematous pyelonephritis.
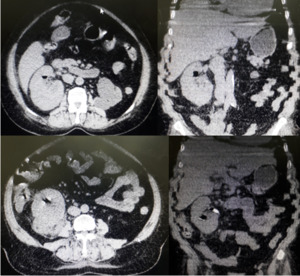
Fig. 3: 35 year-old female patient not diabetic presented with right loin pain and high grad fever. CT shows emphysematous nephritis and pyelitis with upper ureteric obstructive stone.
Management plan is set according to the general condition of the patient and the severity of the disease.
The management depends on combination between antibiotics,
percutaneous drainage and nephrectomy.
Conservative treatment using percutaneous drainage with antibiotics is indicated as follows:
- Patients with compromised renal function
- Early cases associated with gas in the collecting system alone and patient is in otherwise in stable condition.
- Class 1 and class 2 EPN.
- Class 3 and class 4 EPN - In the presence of fewer than 2 risk factors (e.g.,
thrombocytopenia,
elevated serum creatinine levels,
altered sensorium,
shock).
Antibiotic empiric regimen should be broad spectrum and target Gram-negative bacteria.
The presence of more than one organism might necessitate the use of dual antibiotics and take into account individual patient characteristics and local patterns of antibiotic resistance.
Nephrectomy is indicated as follows:
- No access to percutaneous drainage or internal stenting (after patient is stabilized)
- Gas in the renal parenchyma or "dry-type" EPN
- Class 3 and class 4 EPN - In the presence of two or more risk factors .
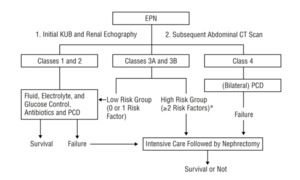
Fig. 5: The flowchart for management of emphysematous pyelonephritis (EPN) according to the clinicoradiological classification. Asterisk indicates the presence of 2 or more of the following risk factors: thrombocytopenia, acute renal failure, disturbance of consciousness, and shock. KUB indicates kidneys, ureter, and bladder (plain abdominal radiograph); CT, computed tomography; and PCD, percutaneous catheter drainage.
References: Huang J, Tseng C. (2000) Emphysematous Pyelonephritis: Clinicoradiological Classification, Management, Prognosis, and Pathogenesis. Arch Intern Med. ;160(6):797–805. doi:10.1001/archinte.160.6.797
Guided percutaneous drainage seems to be as an effective way in decreasing the mortality and morbidity.
it is effective in cases where gas is in the collecting system and not invading the parenchyma or it is confined to the perinephric space.




")
 according to the clinicoradiological classification. Asterisk indicates the presence of 2 or more of the following risk factors: thrombocytopenia, acute renal failure, disturbance of consciousness, and shock. KUB indicates kidneys, ureter, and bladder (plain abdominal radiograph); CT, computed tomography; and PCD, percutaneous catheter drainage. References: Huang J, Tseng C. (2000) Emphysematous Pyelonephritis: Clinicoradiological Classification, Management, Prognosis, and Pathogenesis. Arch Intern Med. ;160(6):797–805. doi:10.1001/archinte.160.6.797")