In our experience,
the rate of B1-lesions is very low,
comparable with the one reported in previously published papers [11].
However,
even if the rate is very low,
a diagnosis of B1-lesion is worrisome for the patient and challenging for the breast radiologist.
What to do next? Such a question is highly relevant,
since in our population the rate of breast cancers diagnosed after a diagnosis of B1-lesion was significant (21.2%).
Notably,
our rate of malignant lesions was higher than the one reported by Rakha and colleagues [11].
However,
their paper was focused on screen-detected lesions,
while we considered both symptomatic and screening patients.
Therefore,
the prevalence of malignant lesion had to be higher.
In our experience,
the only two features significantly different between Breast Cancer and Non Breast Cancer groups were the degree of suspicion according to BIRADS and the presence of cellular atypias.
As for the degree of suspicion,
we found that lesions scored ≥R4b were significantly associated with malignancy,
coherently with published papers and international guidelines [3] (Fig. 3),
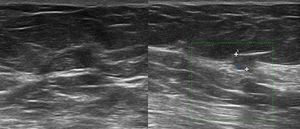
Fig. 3: Sixty-two year-old patient recalled from screening for a mass on the left upper-outer quadrant. Ultrasound examination showed a 5 mm mass with indistinct margins and signs of vascularization at Power Doppler (U4b), which was biopsied with histological result of "insufficient material". The re-biopsy was diagnostic for “infiltrating ductal carcinoma”.
while lesions scored ≤R4a were usually benign (Fig. 4).
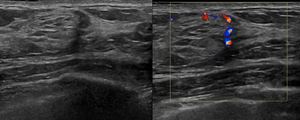
Fig. 4: Sixty-nine year-old patient recalled from screening for a small mass on the left upper-outer quadrant. Ultrasound examination revealed a hypoechoic mass of 9x8 mm, with indistinct margins, with signs of vascularization at Power Doppler (U4a), which was biopsied. The histological diagnosis was "normal mammary parenchyma". Because of imaging-histology discordance the lesion underwent surgical excision, with final diagnosis of “mammary parenchyma with adenosis and stromal fibrosis”.
This finding strengthen the role of the breast radiologist in the setting of the diagnosis of B1-lesions,
since their management relies mainly upon their degree of suspicion,
attributed by the radiologist.
The presence of cellular atypias was significantly associated with malignancy,
too.
It is noteworthy that,
according to literature [1,
2],
a lesion with atypical cells should not be assessed as B1.
However,
it is known [12] that in some cases pathologists are influenced by the radiological features or by the multidisciplinary discussion,
rather than just using the histological features.
This finding too strengthen the role of the breast radiologist,
who has to carefully interpret the pathological report,
deepening equivocal findings such as the presence of atypical cells in a lesion classified as B1.
Interestingly,
malignancy was associated with BI-RADS ≥R4b and/or presence of atypical cells in 83.3% (15/18) of cases (p<0.0001); the remaining 3/18 malignancies were ≤10mm.
Therefore,
even if in our experience the size was not significantly associated with malignancy,
a diameter ≤10mm should be considered an additional warning size.
No other features assessed (Table 1)
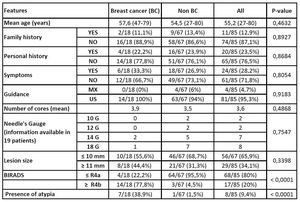
Table 1: Features assessed in Breast Cancer and in Non Breast Cancer group, with p-values.
were significantly associated with breast cancer.
In conclusion: B1-lesions are infrequent,
but their management is crucial and relies completely on the breast radiologist.
Lesions scored ≥R4b and/or with presence of atypical cells need further assessment,
while small lesions (≤10mm) should be considered carefully.

, which was biopsied with histological result of "insufficient material". The re-biopsy was diagnostic for “infiltrating ductal carcinoma”.")
, which was biopsied. The histological diagnosis was "normal mammary parenchyma". Because of imaging-histology discordance the lesion underwent surgical excision, with final diagnosis of “mammary parenchyma with adenosis and stromal fibrosis”.")
