ECR 2019 / C-3213
Breast lesions histologically classified as B1 after percutaneous biopsy: which are the features associated with malignancy?
Congress:
ECR 2019
Poster Number:
C-3213
Type:
Scientific Exhibit
Keywords:
Breast, Interventional non-vascular, Oncology, Mammography, Ultrasound, Percutaneous, Biopsy, Vacuum assisted biopsy, Sampling, Cancer, Neoplasia
Authors:
M. Lorenzon, P. Conte, A. Linda, V. Londero, R. Girometti, C. Zuiani; Udine/IT
DOI:
10.26044/ecr2019/C-3213
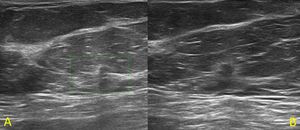
 was found. Histological diagnosis was “normal mammary parenchyma” (A). At 6 months follow-up (B) the lesion was re-biopsied because of a small increase in size and because of the presence of perilesional hyperechoic halo. The final histological diagnosis was "infiltrating ductal carcinoma".")
Fig. 1:
Fifty-nine year-old patient with recent retraction of the right nipple....
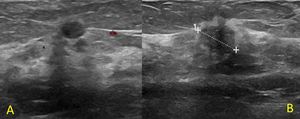
 was found. The histological diagnosis was "normal mammary parenchyma" (A). At 6-months follow-up no changes were noted. At 24-months follow-up (B) the lesion appeared hypoechoic, with irregular shape and indistinct margins (U5); at re-biopsy it resulted an "infiltrating ductal carcinoma".")
Fig. 2:
Sixty-four year-old patient recalled from screening for a small mass in the...

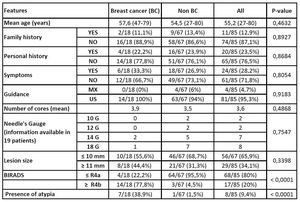
Table 1:
Features assessed in Breast Cancer and in Non Breast Cancer group, with...
, which was biopsied with histological result of "insufficient material". The re-biopsy was diagnostic for “infiltrating ductal carcinoma”.")
Fig. 3:
Sixty-two year-old patient recalled from screening for a mass on the left...
, which was biopsied. The histological diagnosis was "normal mammary parenchyma". Because of imaging-histology discordance the lesion underwent surgical excision, with final diagnosis of “mammary parenchyma with adenosis and stromal fibrosis”.")
Fig. 4:
Sixty-nine year-old patient recalled from screening for a small mass on the...