PAROTID GLAND IMAGING
Imaging exams are an important tool in the evaluation of parotid enlargement.
-Conventional radiography
Radiography may be helpful in the detection of calculi,
but only 20% of the calculi are radiopaque.
This imaging technique can also show calcification and bone invasion but has been replaced by other radiologic modalities.
-Ultrasound (US)
US is an important tool in the evaluation of the major salivary glands.
It does not use ionizing radiation and also enables guidance of fine needle aspiration cytology.
In the parotid assessment,
US allows differentiation of solid from cystic masses,
detection of intraparotid nodes and of ductal dilatation.
However,
US is limited to assess deeper masses.
Normal parotid parenchyma is homogenous and hyperechoic,
when compared to adjacent muscles (Fig. 1).
-Computed tomography (CT)
CT is particularly important when lithiasis is suspected and is also relevant to detect adjacent bone lesions.
In children,
the parotid gland has the same attenuation of the adjacent soft tissue.
However,
with age,
gradual fatty infiltration occurs and parotid tends to present progressively lower attenuation values.
-Magnetic resonance imaging (MRI)
MRI is a good modality to evaluate parotid (Fig. 2),
especially in case of tumoral masses,
namely in defining its extension and margins.
It is the best technique to detect invasion of the meninges and adjacent nerves such as facial,
trigeminal,
hypoglossal and lingual nerves.
These parameters are best depicted on T1-weighted images (WI) with fat-saturation (FS) after gadolinium injection.
PAROTID GLAND DISORDERS
Parotid enlargement can be caused by several disorders (Table 1).
Some conditions can be self-limited,
whereas others have a relapsing course.
Table 1: Differential diagnosis of parotid gland enlargement.
Infectious disorders
Patients typically present with painful parotid swelling,
which is commonly bilateral.
Imaging is usually not requested,
as the diagnosis is clinical.
If requested,
imaging features are non-specific.
Parotid parenchyma appears heterogeneous (Fig. 3) and with increased blood flow.
Regional and intraparotid enlarged lymph nodes may be present.
On US,
small hypoechoic areas,
representing secretions foci and intraparotid lymph nodes can be seen.
On MRI,
the gland can show high signal intensity on T2-WI,
if edema predominates,
or low signal,
if cellular infiltration prevails.
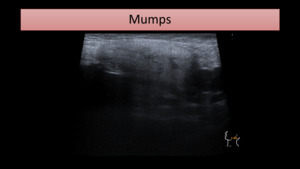
Fig. 3: US image shows an enlarged and heterogeneous parotid gland. Similar features were found on the contralateral gland.
Up to 5-10% of HIV-infected patients have bilateral parotid enlargement,
which may be caused by hyperplastic lymphadenopathy,
due to multiple benign lymphoepithelial cysts or by diffuse infiltrative lymphocytosis syndrome.
US demonstrates large intraparotid lymph nodes and small to medium cysts,
seen as anechoic areas,
that may show internal septa and debris.
CT and MRI show enlarged glands,
with multiple nodes and cysts,
respectively seen as near-water density on CT and high signal intensity on T2-WI (Fig. 4).
Enlarged cervical nodes may also be seen.
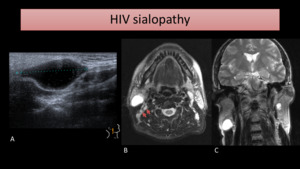
Fig. 4: US (A) of the right parotid gland shows a large lymphoepithelial cyst. MR images of the same patient show bilateral hyperintense cystic lesions on T2-WI with FS (B) and T2-WI (C). Also, several cervical lymph nodes were present, some of them seen on image B (arrows).
- Acute bacterial parotitis
Bacterial parotitis is more common in children,
especially in cases of immune deficiency and prematurity.
Besides parotid enlargement and subcutaneous fat-stranding (Fig. 5),
abscesses may be seen within the parotid gland,
typically formed from necrotic lymph nodes.
Abscesses are depicted as collections with rim enhancement on CT.
Fig. 5: CT image shows left parotid enlargement (encircled) with pronounced subcutaneous fat-stranding.
Cystic lesions
Examples of cystic lesions that can cause parotid enlargement include mucous retention cyst (Fig. 6),
lymphoepithelial cyst,
first branchial cleft cyst and pseudocyst.
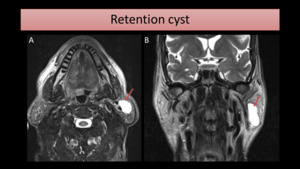
Fig. 6: MR study shows a large cystic lesion (arrow) on the left parotid gland, hyperintense on axial T2-FS (A) and T2-WI coronal image (B). The fine needle aspiration cytology revealed it was a retention cyst.
Sialolithiasis
Lithiasis is the second most common cause of sialadenitis.
It is most frequently seen on submandibular glands,
however,
up to 20% of salivary calculi are found in parotid.
Patients present with diffuse or focal parotid enlargement,
usually unilateral.
US is an important tool as a first-line assessment of ductal ectasia and lithiasis.
However,
small calculi (inferior to 2-3 mm) may not be detected.
CT provides a good detection of calculi and assessment of adjacent gland (Fig. 7).
MRI allows detailed characterization of the ductal system and glandular parenchyma,
in a non-invasive way.
Besides calculi,
imaging may show associated features,
such as ductal ectasia,
heterogeneous gland parenchyma and possible abscesses.
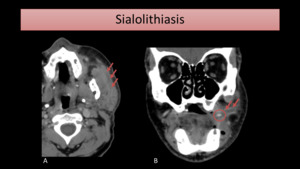
Fig. 7: CT images show a stone (circle) causing Stensen´s duct dilatation (arrows) and parotitis.
Chronic recurrent parotitis
Chronic recurrent parotitis may cause relapsing episodes of inflammatory parotid enlargement.
Its etiology is unknown,
but some proposed causes include recurrent infections or autoimmune diseases.
With time,
the parotid usually tends to become atrophic.
US demonstrates tiny anechoic spaces,
due to sialectasis,
and small round hypoechoic nodes,
representing secretions and intraparotid lymph nodes.
Calcifications are better seen on CT.
MRI may show diffuse gland enlargement,
with small areas of high signal on T2-WI (Fig. 8).
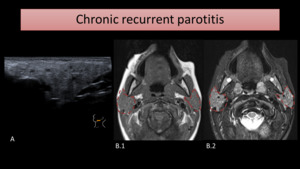
Fig. 8: US (A) shows parotid enlargement with small anechoic spaces, in a patient with recurrent infectious parotitis. MR images of a different patient show enlarged and heterogeneous parotid glands, as seen on T1-WI (B.1) and T2-WI (B.2). On the latter image, tiny areas of high signal are seen.
Autoimmune disorders
Sjögren’s disease is characterized by destruction of exocrine glands,
due to a lymphocytic and plasma cell infiltration.
Up to 55% of patients with this condition have bilateral parotid enlargement.
Patients with Sjögren's disease have a higher risk of calculi formation and a 44-fold increased risk of lymphoma,
mainly marginal zone B-cell lymphoma.
On US,
parotid glands are heterogeneous,
revealing hypoechoic or anechoic areas,
which represent sialectasis and destroyed acini (Fig. 9).
Doppler may show increased parenchyma blood flow.
On CT,
the gland is enlarged,
with high attenuation and abnormal enhancement.
MRI shows a typical pattern in advanced cases,
named salt and pepper or honeycombing – consisting of scattered areas of high signal on T2-WI,
mixed with foci of low signal.
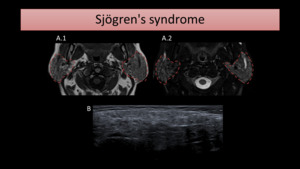
Fig. 9: Axial MR images (A) show enlarged and heterogeneous parotid glands, with scattered areas of low signal on T1-WI (A.1) and high signal intensity on T2-WI with FS (B.2). On US (B), the parotid gland is heterogeneous, revealing small anechoic and hypoechoic nodules.
Parotid gland can be affected in up to 30% of the patients with this disease.
Similar to Sjögren's disease,
patients have a higher risk of calculi formation.
Imaging features are non-specific.
Parotid is enlarged and presents intraglandular nodes,
seen on US,
CT and MRI (Fig. 10).
Enlarged cervical nodes may be seen.
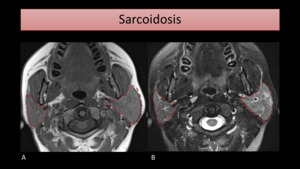
Fig. 10: T1-WI (A) and T2-WI with FS (B) MR images show parotid enlargement (encircled), more prominent on the left, with heterogeneous gland signal intensity, in a patient with known sarcoidosis.
- Granulomatosis with polyangiitis
Parotid enlarged,
either unilateral or bilateral,
may be caused by other granulomatous conditions such as Granulomatosis with polyangiitis.
Parotid involvement occurs in the context of respiratory disease.
Imaging is non-specific.
Parotid parenchyma is enlarged and hyperenhancing.
Sialadenosis
Parotid may be recurrently enlarged by several non-inflammatory conditions.
These include endocrine causes (diabetes mellitus,
hypothyroidism),
alcoholism,
anorexia and medication (such as psychotropic medications).
Its etiology is unknown but it is thought to be associated,
in some degree,
to an autonomic neuropathy process.
Imaging features are non-specific.
Neoplasms
Salivary neoplasms are a morphologically diverse group,
as seen on the WHO histological classification of tumors of the salivary gland,
revised in 2017 (Table 2).
The rate of malignancy decreases as the size of the gland increases.
Thus,
most of the parotid tumors are benign,
either pleomorphic adenoma or Warthin tumor,
and only less than 30% of the masses found in parotid glands are malignant.
It's not easy to differentiate the several types of tumors that involve the parotid gland because they share clinical and imaging features.
On imaging,
features that suggest malignancy include ill-defined margins with invasion of other cervical planes and cervical lymphadenopathy.
1.
Pleomorphic adenoma
Pleomorphic adenoma (PA) represents 40% of benign parotid neoplasms.
PA is more common in middle-aged women,
in their 4th and 5th decades of life.
It presents typically as a solitary,
slow-growing and painless mass.
This tumor is depicted on imaging as a well-defined and encapsulated mass.
Necrosis and hemorrhage may be seen in larger neoplasms.
US demonstrates a lobulated mass,
hypoechoic to isoechoic when compared to adjacent parenchyma,
possible with associated posterior acoustic enhancement.
On Doppler,
central hipovascularity with peripheral vascularity is seen.
CT depicts a low attenuating mass with variable enhancement.
Calcifications may be seen and are common.
PA is seen on MRI as a homogeneous mass,
with low signal on T1-WI and high signal on T2-WI.
The capsule is hypointense on T2-WI.
After gadolinium injection,
mild enhancement may occur (Fig. 11)
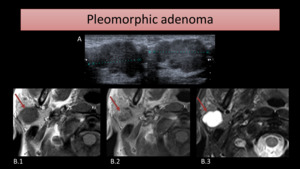
Fig. 11: US images (A) show a lobulated and hypoechoic mass. MRI images of another patient show a homogeneous mass (arrow) on the right parotid gland, hypointense on T1-WI (B.1) and hyperintense on T2-WI (B.3). A low-signal intensity halo is seen on image B.3, representing the tumor’s capsule. After gadolinium injection (B.2), the mass mildly enhances.
2.
Warthin tumor
Warthin tumor (WT) is a benign neoplasm that does not occur in other salivary glands apart from the parotid.
It is more common in men,
in their 5th and 6th decades of life.
It is associated with smoking and typically presents as a painless mass.
WT appears on US as an oval,
well-defined and hypoechoic mass,
which may be partial or completely cystic.
Usually,
high vascularization is seen on Doppler.
On MRI,
the cystic component is seen as a high signal area on T2-WI (Fig. 12).
The mass typically is hypointense on T2-WI.
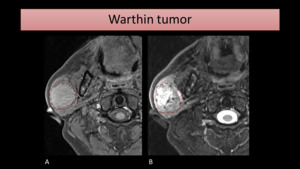
Fig. 12: MR images show a mass (encircled) on the right parotid gland, slightly hyperintense on T1-FS (A) and heterogeneous on T2-WI with FS (B), due to the presence of scattered cystic areas.
One must suspect of WT if multiple or bilateral masses are seen on parotid (Fig. 13),
since the tumor is bilateral in up to 10% of the cases.
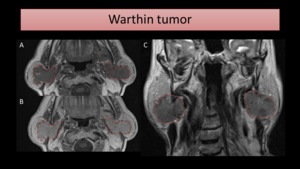
Fig. 13: MR images show bilateral parotid masses, hypointense on T1 (A) and T2-WI (C). After gadolinium injection (B), there is homogeneous enhancement.
1.
Mucoepidermoid carcinoma
Mucoepidermoid carcinoma (MC) is the most common malignant tumor found in the parotid gland.
It is more common in adults,
between 30 and 50 years of age,
typically presenting as a slow-growing mass.
Imaging features vary according to the tumor grade,
which can be divided as low,
intermediate and high-grade.
Slow-grade tumors present imaging features similar to those of benign neoplasms.
High-grade MC,
on the other hand,
are more heterogeneous,
tend to present poorly defined margins and heterogeneous enhancement.
On MRI (Fig. 14),
a mass with low to intermediate signal on T1 and T2-WI may be seen.
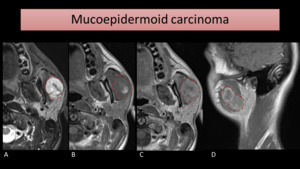
Fig. 14: MRI images show a mass on the left parotid gland invading the masseter muscle. This mass had a very fast growth, which increases the suspicion of malignancy. The fine needle aspiration cytology revealed it was a high-grade mucoepidermoid carcinoma. It shows an intermediate signal intensity on T1-WI (B) and an unexpected high signal intensity on T2-WI (A). After gadolinium (C and D), enhancement is seen.
2.
Lymphoma
Primary lymphoma of the parotid,
a mucosa-associated lymphoid tissue (MALT) lymphoma,
is rare.
Secondary lymphoma is also rare but still more frequent than the primary one.
Patients with Sjögren's disease,
HIV and chronic sialadenitis are at higher risk of parotid lymphoma.
The typical presentation is painless enlargement of the gland,
which can be either unilateral or bilateral.
A focal or diffuse involvement of the gland may be seen,
along with enlarged intraparotid lymph nodes.
US shows several or a solitary hypoechoic lesion,
which may present internal septa.
MRI demonstrates intermediate signal on T1 and T2-WI,
and uniform enhancement on CT and MRI.
IgG4 – related diseases
In the head and neck,
salivary glands are the most common site of affection and two different conditions can be seen: Mikulicz syndrome and chronic sialadenitis (Küttner tumor).
It is estimated that 40% of the patients with IgG4-related pancreatitis,
also have salivary gland involvement.
For the diagnosis of Mikulicz disease,
enlargement of at least two of the three major salivary glands and/or lacrimal glands must be present.
It was initially described as a subtype of Sjögren’s,
as both show lymphocytic infiltration of the affected glands.
On CT,
enlarged parotid with homogenous attenuation and enhancement may be seen.
MRI shows low-signal intensity on T2-WI due to fibrosis and low-signal on T1-WI.
Küttner tumor is a chronic sclerosing sialadenitis of the salivary glands,
mainly the submandibular,
causing unilateral or bilateral enlargement.
However,
other salivary glands including parotid may be affected.
Imaging is similar to Mikulicz disease,
but a higher degree of fibrosis may be seen.
IgG4-related diseases must be suspected as a cause of parotid enlargement when there is associated multiorgan involvement,
namely pancreatic affection.
Vascular malformations
Vascular malformations,
namely the venous and lymphatic types,
may be a cause of parotid enlargement,
especially in children (Fig. 15).
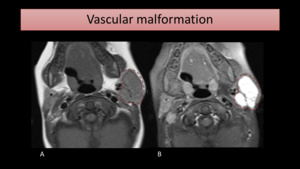
Fig. 15: T1-WI and T1-FS with gadolinium MR images show an enhancing lesion (encircled) causing left parotid enlargement, with a small flow-void inside, consistent with a venous vascular malformation.
Lymph nodes
Enlarged intraparotid lymph nodes may be the cause of parotid enlargement and may be caused by extraparotid tumor dissemination,
most common,
by dermatologic tumors or upper airway malignancies.
Other causes (rare)
- Radiation
- Polycystic disease
- Pneumoparotid
- Kimura disease
Conditions that mimic parotid enlargement
One condition that may mimic a parotid enlargement is masseter hypertrophy.
This can be seen on MRI,
as an enlarged masseter with normal signal intensity (Fig. 16).

Fig. 16: T1-WI MR image shows assimetric masseter hypertrophy on the left (encircled), simulating parotid enlargement.
An accessory parotid gland may also simulate a parotid enlargement (Fig. 17).
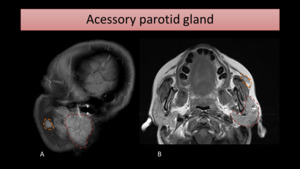
Fig. 17: MR sagittal T1-WI with FS (A) and axial T1-WI (B) show an acessory parotid gland (encircled in orange), located anteriorly to the main left parotid gland (encircled in red).
Some extra-parotid tumors may also be mistaken for parotid disorders,
namely peripheral nerve sheath neoplasms,
which include neurofibroma and schwannoma.


 seen on axial MR images: T1-WI (A), T1-WI with gadolinium (B) and T2-WI (C).")

 of the right parotid gland shows a large lymphoepithelial cyst. MR images of the same patient show bilateral hyperintense cystic lesions on T2-WI with FS (B) and T2-WI (C). Also, several cervical lymph nodes were present, some of them seen on image B (arrows).")
 with pronounced subcutaneous fat-stranding.")
 on the left parotid gland, hyperintense on axial T2-FS (A) and T2-WI coronal image (B). The fine needle aspiration cytology revealed it was a retention cyst.")
 causing Stensen´s duct dilatation (arrows) and parotitis.")
 shows parotid enlargement with small anechoic spaces, in a patient with recurrent infectious parotitis. MR images of a different patient show enlarged and heterogeneous parotid glands, as seen on T1-WI (B.1) and T2-WI (B.2). On the latter image, tiny areas of high signal are seen.")
 show enlarged and heterogeneous parotid glands, with scattered areas of low signal on T1-WI (A.1) and high signal intensity on T2-WI with FS (B.2). On US (B), the parotid gland is heterogeneous, revealing small anechoic and hypoechoic nodules.")
 and T2-WI with FS (B) MR images show parotid enlargement (encircled), more prominent on the left, with heterogeneous gland signal intensity, in a patient with known sarcoidosis.")
 show a lobulated and hypoechoic mass. MRI images of another patient show a homogeneous mass (arrow) on the right parotid gland, hypointense on T1-WI (B.1) and hyperintense on T2-WI (B.3). A low-signal intensity halo is seen on image B.3, representing the tumor’s capsule. After gadolinium injection (B.2), the mass mildly enhances.")
 on the right parotid gland, slightly hyperintense on T1-FS (A) and heterogeneous on T2-WI with FS (B), due to the presence of scattered cystic areas.")
 and T2-WI (C). After gadolinium injection (B), there is homogeneous enhancement.")
 and an unexpected high signal intensity on T2-WI (A). After gadolinium (C and D), enhancement is seen.")
 causing left parotid enlargement, with a small flow-void inside, consistent with a venous vascular malformation.")
, simulating parotid enlargement.")
 and axial T1-WI (B) show an acessory parotid gland (encircled in orange), located anteriorly to the main left parotid gland (encircled in red).")
