We present a range of interesting cases which demonstrate the key CT imaging features of urological complications and discuss the importance of interventional radiology in such management.
Early CT imaging is essential to assess:
- Size and location of any abdomino-pelvic collections
- Contrast extravasation on excretory phase suggesting anastamotic leak or bladder perforation
- Hydroureteronephrosis
- Evidence of active haemorrhage requiring prompt arterial embolisation or surgical intervention
- Small bowel dilatation
- Signs of bowel injury
- Placement of ureteric stents,
nephrostomy catheters and surgical drains
Case 1: Large uretero-ileal anastamotic leak
50 year old male underwent a robotic assisted cystectomy for muscle invasive TCC post neoadjuvent chemotherapy. 5 days post-operatively,
he developed abdominal distension,
raised inflammatory markers and significant output of urine from the pelvic drain.
CT demonstrated dilated small bowel loops consistent with paralytic ileus and a large fluid collection extending into the pelvis consistent with a uretero-ileal anastamotic leak.

Fig. 1: Case 1: Uretero-ileal anastamotic leak.
Contrast enhanced CT demonstrates dilated small bowel loops suggestive of paralytic ileus. Large abdomino-pelvic fluid collection consistent with urine leak.
Patient also suffered a pulmonary embolism requiring anticoagulation.
In order to achieve urinary diversion,
rather than percutaneous nephrostomy,
bilateral retrograde ureteric pigtail stents were placed via the ileal conduit,
exiting into the stoma bag.
Technique is illustrated below:
Interventional radiology technique:
Careful placement of 5F vascular sheath into the conduit,
anchoring this to the surgical drape with a clip for stability.
Conduitogram performed to delineate anatomy and allow navigation with wire-catheter combination.
5F biliary manipulation catheter and angled hydrophilic guidewire used to cross anastamoses and retrograde pyelograms performed to confirm position of collecting systems.
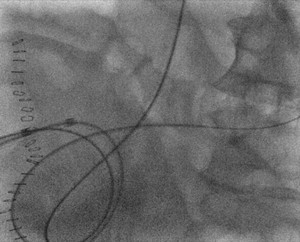
Fig. 2: Case 1 - Bilateral cannulation of ureters via ileal conduit

Fig. 3: Case 1 - Right retrograde ureteric stent placed.
8F 24 cm length JJ ureteric pigtail stents sited over stiff Amplatz guidewires,
with distal pigtails lying outside stoma to provide urinary diversion.
Conduit was also decompressed with a 16F Foley catheter.

Fig. 4: Case 1 - Bilaterally sited ureteric stents achieving urinary diversion
Patient made an excellent recovery and a follow up CT in 10 days revealed complete resolution of the large leak.
A conduitogram was performed to ensure there was no residual leak and the stents subsequently withdrawn.

Fig. 5: Case 1 - Follow up CT demonstrates the balloon of Foley catheter lying within the ileal conduit. Complete resolution of the anastamotic leak.
Case 2: Large extraperitoneal haematoma following robotic assisted radical prostatectomy (RALP)
56 year old male who underwent a difficult prostatectomy attended two weeks post operatively for a check cystogram.
He described vague pelvic discomfort and symptoms of urgency despite urethral catheterisation.
Cystogram revealed an elongated appearance of the urinary bladder with irregular indentation of the left bladder wall suggestive of extrinsic compression.

Fig. 6: Case 2 - Cystogram performed via indwelling urethral catheter revealing an unusually elongated bladder with extrinsic indentation of the left bladder wall.
Contrast enhanced CT demonstrated a large extraperitoneal haematoma compressing the urinary bladder.

Fig. 7: Case 2 - Axial CT image demonstrating large extraperitoneal haematoma. Urinary bladder is opacified with contrast and is displaced posteriorly.
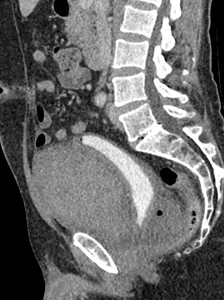
Fig. 8: Case 3 - Sagittal image demonstrating the extraperitoneal location of the large post-operative haematoma. Posterior to the bladder, a small fluid collection is also noted within the surgical bed. Urinary bladder is compressed and elongated.
He required a lower midline laparotomy to evacuate the large haematoma and subsequently made an uncomplicated recovery.
Case 3 - Post operative lymphocele and fistulation between neo-bladder and anterior abdominal wall
63 year old male underwent a robotic cystectomy,
extended pelvic lymph node dissection and neobladder formation for recurrent TCC.
10 days post-op he demonstrated signs of sepsis and underwent contrast enhanced CT for evaluation.

Fig. 9: Case 4 - Bilateral pelvic fluid collections adjacent to the surgical clips consistent with lymphoceles following extended lymph node dissection.
In view of his worsening sepsis and raised inflammatory markers,
he underwent CT guided drainage of suspected infected lymphoceles.

Fig. 10: Case 4 - CT guided puncture with 18G 3 part needle to access left pelvic fluid collection.
The drainage successfully treated his sepsis,
however after 8 days he developed a wound dehiscence with copious volumes of urine draining from the wound.
A CT demonstrated a fistulous tract between his neobladder and dehisced wound.
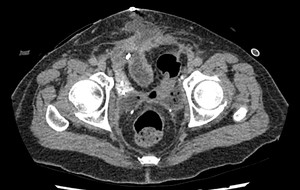
Fig. 11: Case 4 - Fistulous tract between neobladder and dehisced anterior abdominal wound with surrounding inflammatory changes.
Patient underwent bilateral percutaneous nephrostomy placement to achieve urinary diversion.
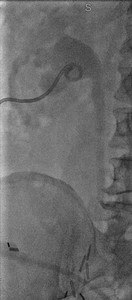
Fig. 12: Case 4 - Percutaneous nephrostomy placement for urinary diversion to allow fistula to seal.
A subsequent CT after 10 days revealed satisfactory closure of the fistulous tract and the patient went on to make a good recovery.

Fig. 13: Case 4 - Follow up excretory CT urogram revealing closure of fistula.
Case 4 - Extraperitoneal bladder perforation post TURBT
63 year old female who present with frank haematuria underwent a transurethral resection of TCC arising from the left lateral bladder wall.
Postoperatively she developed severe pelvic pain.
A CT cystogram was performed which revealed an extraperitoneal bladder perforation.

Fig. 14: Case 5 - Ct cystogram demonstrating left sided extraperitoneal bladder perforation post TURBT

Fig. 15: Case 5 - Ct cystogram demonstrating left sided extraperitoneal bladder perforation post TURBT
She was managed conservatively with a urinary catheter and antibiotics.
10 days later she underwent a cystogram which demonstrated irregularity at the site of the tumour but no evidence of contrast extravasation.
She subsequently made a good recovery with no evidence of tumour recurrence.
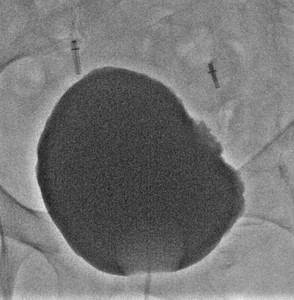
Fig. 16: Case 5 - Cystogram reveals irregularity of the left bladder wall at the site of resection but no evidence of extravasation.
Case 5 - Superficial wound collection post open nephrectomy
62 year old male underwent an uncomplicated right open nephrectomy for a large RCC.
5 days post-operatively he developed a large fluctuant swelling over his right flank with overlying erythema.
CT revealed a large gas/fluid collection consistent with an infected subcutaneous collection.

Fig. 17: Case 6 - Right flank gas/fluid collection post nephrectomy with inflammatory fat stranding of the subcutaneous fat.
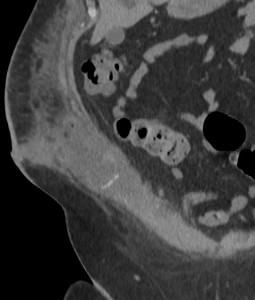
Fig. 18: Case 6 - Right flank gas/fluid collection post nephrectomy with inflammatory fat stranding of the subcutaneous fat.
He underwent US guided percutaneous drainage of the collection using Seldinger technique and placement of a 12F pigtail drainage catheter.
This drained > 500 mls frank pus following which he made an uncomplicated recovery.
Case 6 - Anastamotic leak following RALP
73 year old male was readmitted 2 days following robotic assisted prostatectomy with severe abdominal pain and raised inflammatory markers.
CT urogram demonstrated a large anastamotic urine leak.

Fig. 19: Case 7 - Excretory phase CT urogram reveals large leak around the bladder anastamosis. Contrast extravasation is seen encircling and pooling around the anastamotic site.
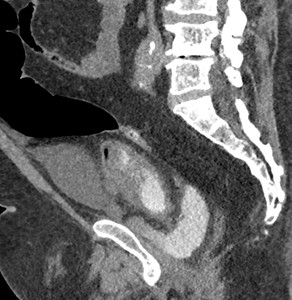
Fig. 20: Case 7 - Excretory phase CT urogram reveals large leak around the bladder anastamosis. Contrast extravasation is seen encircling and pooling around the anastamotic site.
Patient underwent percutaneous CT guided drainage of the anterior fluid collection given his raised inflammatory markers and pyrexia.
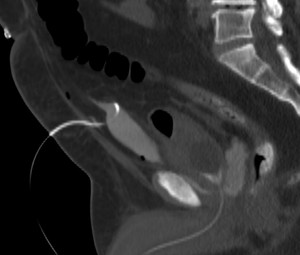
Fig. 21: Case 7 - CT guided drainage of anterior fluid collection with 8.5F pigtail catheter
10 days later he attended for a check cystogram which revealed a large persisting leak posterior to the anastamosis.
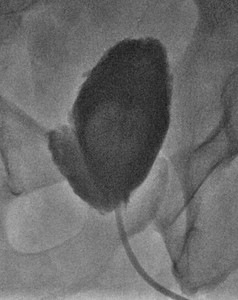
Fig. 22: Case 7 - Follow up cystogram revealing persisting posterior anastamotic leak.
He underwent a prolonged period with indwelling urinary catheter and subsequently made a good recovery.



