I-Cholangiocarcinoma classifications
- Cholangiocarcinomas may occur at any segment of the bile duct from the terminal ductules to the ampulla of Vater.
Therefore,
they can be classified anatomically as intrahepatic or peripheral (6- 8% of cases),
perihilar also called Klatskin tumors (50- 67% of cases),
and extrahepatic (27- 42%) ( Fig. 1 ).
The reference point to differentiate intrahepatic from perihilar CC is the second order bile ducts.
Intrahepatic cholangiocarcinomas arise from beyond second-order bile ducts. Tumors originating in the right,
left or common hepatic conduits are considered perihilar.
From the insertion of the cystic conduit,
they are considered distal.
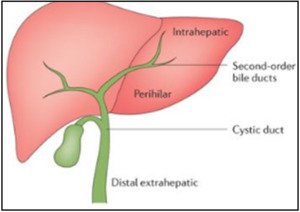
Fig. 1: Anatomical classification of cholangiocarcinomas
References: Nature Reviews 2016
- Perihilar lesions also called Klatskin tumors have been further divided by Bismuth and Corlette,
according to the extent of ductal involvement,
into four types( Fig. 2 ):

Fig. 2: Bismuth- Corlette classification of Klatskin tumors.
References: Blechacz. Cholangiocarcinoma: Current Knowledge and New Developments. Gut and Liver 2017; 11(1): 13- 26.
-type I: the tumor is limited the common hepatic duct,
below the level of the confluence of the right and left hepatic ducts.
-type II: the tumor involves the confluence of the right and left hepatic ducts.
-type IIIa: type II tumor extending to the bifurcation of the right hepatic duct.
-type IIIb: type II tumor extending to the bifurcation of the left hepatic duct.
-type IV: type II tumor extending to the bifurcations of both right and left hepatic ducts or tumor with multifocal involvement.
- On the basis of the Japanese Liver Cancer Group classification, cholangiocarcinoma can also be classified into three types on the basis of morphologic features ( Fig. 3 ): mass-forming (exophytic),
periductal infiltrating,
and intraductal(polypoid).
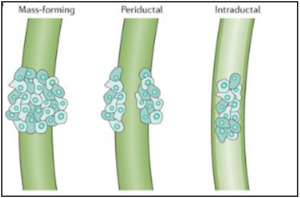
Fig. 3: Morphological classification of cholangiocarcinomas
References: Nature Reviews 2016
- The infiltrating type is the most common in the perihilar region.
II- Imaging spectrum of cholangiocarcinoma
- Advances in imaging techniques,
especially CT and MRI techniques used independently or in combination,
have led to an accurate diagnosis and evaluation of cholangiocarcinomas in preparation for advanced surgical procedures and treatment planning.
- Imaging plays a crucial role in non-invasive diagnosis and characterization of cholangiocarcinomas,
pre-therapeutic staging,
and assessment of resectability,
and screening of high-risk patients for early detection.
A-Computed tomography (CT) imaging
- CT is performed in up to 90% of suspected CC,
offering the opportunity of assessing the full extension of the tumor and determining potential surgical resectability.
B-Magnetic resonance imaging (MRI)
- According to current guidelines,
MRI is the modality of choice for the diagnosis and staging of CC.
in comparison to other imaging techniques,
MRI enables higher tissue contrast and leads to improved tumor detectability.
- A typical MRI protocol encompasses magnetic resonance cholangiopancreatography (MRCP),
conventional T1- and T2-weighted sequences,
diffusion-weighted imaging (DWI) and dynamic contrast-enhanced (DCE) MRI.
MRCP is a non-contrast MRI technique for assessing the biliary system.
It is the most accurate non-invasive imaging technique that allows accurate tumor assessment in both proximal and distal bile ducts.
MRCP sequences are usually acquired using a combination of thick-slab radial T2 sequences which provide a good overview of the biliary system with good suppression of the surrounding tissue,
and thin 3D T2 sequences which provide high spatial resolution allowing the detection of small abnormalities in the bile ducts such as strictures.DWI,
DCE-MRI and late-phase sequences are helpful in the assessment of extra-ductal tumor growth as well as in the depiction of tumor masses within dilated bile ducts.
III-Imaging features of cholangiocarcinomas
A. Intrahepatic and peri-hilar cholangiocarcinomas
1. Mass-forming pattern
- It’s the most common type of intrahepatic CC
a. Intrahepatic exophytic CC
- At CT,
intrahepatic CC manifests as a hypoattenuating large mass with irregular margins.
- In MRI the mass is hypointense relative to normal liver on T1-weighted images.
In T2-weighted images,
it is usually isointense or slightly hyperintense in 2/3 and markedly hyperintense in 1/3 of patients.
- After intravenous administration of contrast material in CT or paramagnetic agent in MRI,
incomplete slight rim-like contrast enhancement can be seen at the early phase with a progressive and concentric filling of contrast at the delayed phase.
The degree of enhancement of a tumor in the delayed phase image is directly related to the amount of interstitial space in the fibrous stroma.
- Usually,
we can see focal dilatation of intrahepatic bile ducts around the tumor because of obstruction.
Satellite nodules of masses are seen in 65% of patients.
Retraction of the liver capsule may be seen when the lesion is peripheral ( Fig. 4 ).
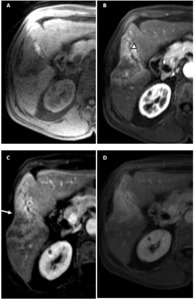
Fig. 4: Exophytic peripheral CC.
T1-W images without (A) and with contrast enhancement in arterial phase (B), venous phase (C) and delayed phase (D) show a typical enhancement pattern in exophytic CC: hypointense masse before contrast administration with incomplete rim enhancement in venous phase and delayed enhancement. Note asymmetric dilation of the peripheral intrahepatic ducts surrounding the mass (arrowheads) and the capsular retraction (white arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
b. Hilar mass-forming CC
- Similar radiological findings to those seen in peripheral mass-forming CC are described: large,
low-attenuation mass with peripheral rim enhancement in the portal phase and delayed enhancement with increasing attenuation in almost 2/3 of patients( Fig. 5 ).
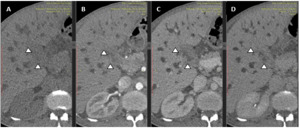
Fig. 5: Exophytic hiliar CC.
CT scan images without contrast (A), in arterial phase (B), portal phase (C) and delayed phase (D) show low attenuation mass at the hepatic hilium before contrast administration with slight peripheral enhancement in the portal phase and homogenous isoattenuating mass in delayed phase.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
- In some cases,
the diagnosis can be challenging because we cannot be sure whether the tumor arises at the main hepatic bifurcation or is a peripheral CC that secondarily invades the hilar area( Fig. 6 ).
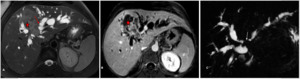
Fig. 6: Exophytic peripheral CC with extension to the hilar plate.
Axial T2- (A) and T1 post-gadolinium- (B) weighted images show a peripheral mass-forming cholangiocarcinoma (*) infiltrating the hilar area with vascular encasement and secondary important intrahepatic bile duct dilatation (red arrow). The magnetic cholangiography (C) shows a signal void (white arrow) at the confluence of the main hepatic ducts.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
2. Infiltrative pattern
- The periductal intrahepatic CC is characterized by tumor infiltration along the bile duct.
a. Peripheral infiltrative CC
- This type of tumor causes segmental dilatation of the bile ducts without visible mass.
This is usually the only sign of the tumor in CT and MRI.
- When the tumor invades the corresponding portal vein,
it can cause lobar or segmental atrophy,
followed by compensatory hypertrophy of the non-affected lobe.
This phenomenon is called the "atrophy-hypertrophy complex".
b. Hilar infiltrative CC
- It is the most common type of hilar CC (over 70% of cases).
It manifests as a dilatation of the intrahepatic bile ducts associated with non-dilated extra-hepatic bile duct.
- CT shows tumoral involvement as an irregular periductal thickening completely obstructing or narrowing a short segment of the biliary tree around the biliary bifurcation.
Periductal thickening is usually iso- hypo enhancing in arterial and portal phases and shows marked enhancement on delayed phase imaging.
- On MRI,
nonunion of the right and left hepatic duct is a typical finding of infiltrating hilar cholangiocarcinoma ( Fig. 7 ).
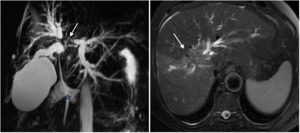
Fig. 7: Infiltrative hiliar CC.
The magnetic cholangiography shows a signal void (white arrow) at the confluence of the main hepatic ducts (left and right), dilated bilateral intahepatic bile ducts and no dilated extrahepatic bile duct (blue marker), consistent with infiltrative hiliar CCA with proximal extension into the right and left hepatic bile ducts (Type IV of Bismuth-Corlette).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
3. Polypoid pattern
- This rare type of tumor has a better prognosis than other CCA.
It manifests as an intraluminal mass with superficial mucosal spreading.
This pattern of cholangiocarcinoma is frequently found in papillary cholangiocarcinomas.
- It’s confined in the lumen of the dilated bile duct without direct tumoral extension to the surrounding liver parenchyma which is different from mass-forming or periductal infiltrating cholangiocarcinoma that typically shows marked infiltration.
This related to the different histological patterns of the tumors.
- It appears as a nodular,
well-defined mass on CT or MR and typically shows hypoattenuating soft-tissue mass relative to the hepatic parenchyma but higher than of the bile with intense enhancement after contrast injection.
The mass is confined within the bile ducts and therefore there is a preservation of the bile duct wall
B. Extrahepatic cholangiocarcinoma
1. Infiltrative pattern
- It is the most common type of CCA involving the extra-hepatic bile duct.
CT scan demonstrates dilatation of intra and extra-hepatic bile ducts to the point where we can see a pronounced thickening of the ductal wall or luminal narrowing.
- Hyperenhancement of the involved common bile duct during the portal phase is the main factor distinguishing malignant from benign strictures ( Fig. 8 ).
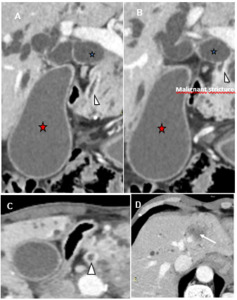
Fig. 8: Infiltrative extrahepatic CC.
Coronal (A, B) and axial (C, D) CT scan images show dilated extrahepatic (blue markers) and cystic bile ducts (red markers) until the intrapancreatic portion of the common bile duct, where there is an hyperattenuated thickened wall (arrowhead). Note satellite nodule in the right hepatic lobe (white arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
2. Polypoid pattern
- It presents as a low attenuation mass within the dilated bile duct,
with similar radiological findings to those seen in polypoid tumors of the hilar area or intrahepatic ducts ( Fig. 9 ).
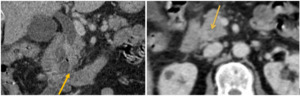
Fig. 9: Polypoid extrahepatic CC.
Axial CT scan contrast-enhanced images show dilated intrahepatic bile ducts, gallbladder and common bile duct until intrapancreatic portion, where there is a nodular soft-tissue mass responsible of a total obliteration of the lumen (yellow arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
III- Preoperative staging and assessment of resectability
- Surgery is the only curative therapy for cholangiocarcinomas.
- The surgical objective for the cure and long-term survival is complete tumor excision with negative histologic margins,
along with the relief of obstruction and restoration of bilio-enteric communication.
- Surgical treatment options are primarily dependent on the tumor site,
the extent of bile duct involvement,
and the relationship of the tumor to critical vascularization in the vicinity.
- The main problem until now has been the poor results of preoperative staging methods in order to separate potentially resectable from non-resectable patients and to avoid unnecessary surgical procedures,
because benefits in terms of survival are only achieved if the tumor is completely resected.
- The following entities preclude curative resection:
*Advanced disease with involvement of the RHD or LHD to the level of the secondary biliary radicles
*Atrophy of one liver lobe with contro-lateral portal vein branch encasement
*Atrophy of one liver lobe with contro-lateral secondary biliary radicle involvement
*Vascular encasement or invasion (proper hepatic artery,
bilateral hepatic arteries,
main portal vein)
*Metastases to lymph nodes,
the peritoneal cavity or distant organs ( Fig. 10 ).
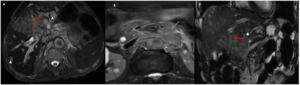
Fig. 10: Non-resectable cholangiocarcinoma.
Axial (A, B) and coronal (C) T2-weighted images show a mass-forming CC infiltrating the biliary confluent and left biliary ducts (Bismuth IIIb) with vascular encasement : thrombosis of the left portal vein and extension to the common and left hepatic arteries (red arrows) with multiple metastatic hepatic nodules (arrowhead) and loco-regional lymph node extension (blue arrows).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
Radial extension of cholangiocarcinoma: Vascular staging
- The vascular extension is either assessed with multidetector CT or gadolinium-enhanced dynamic MRI.
Accurate preoperative assessment of cholangiocarcinoma requires an evaluation of the hepatic artery- right,
left and common hepatic artery ( Fig. 11 ,
Fig. 12 ),
and portal veins- right,
left and main portal vein ( Fig. 13 ).
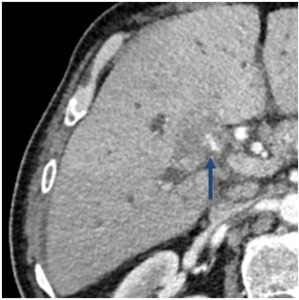
Fig. 11: Arterial infiltration of cholangiocarcinoma.
Axial computed tomography in the arterial phase shows a hilar mass with encasement and infiltration of the right hepatic arteria (blue arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
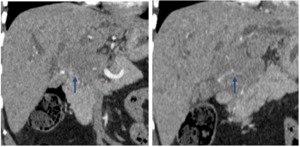
Fig. 12: Arterial infiltration of cholangiocarcinoma.
Coronal CT images in the arterial phase show a hilar mass with encasement and infiltration of the common hepatic arteria (blue arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia

Fig. 13: Portal infiltration of cholangiocarcinoma.
Axial CT contrast-enhanced image in the portal phase shows a hilar mass in the portal confluence (arrowheads) producing biliary dilatation with encasement and infiltration of the main portal vein.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
C. Loco-regional and distant extension of cholangiocarcinoma: Loco-regional lymph node and distant staging
- Multidetector CT helps scrutinize the entire abdomen and pelvis for metastatic spread to lymph nodes ( Fig. 14 ) and distant organs ( Fig. 15 ),
although the sensitivity of CT for lymph node metastases has been found to be low.
- Recently,
with the advent of functional imaging such as positron emission tomography-computed tomography (PET-CT) that allows the study of the whole body,
the need for additional imaging in patients with cholangiocarcinoma has arisen,
in order to rule out distant metastases before radical treatment.
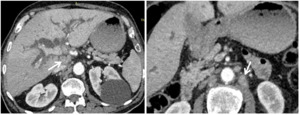
Fig. 14: Loco-regional lymph nodes extension of cholangiocarcinoma.
Axial CT images in the portal phase show a hilar mass in the portal confluence producing biliary dilatation with retroperitoneal and perihilar lymph nodes (white arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
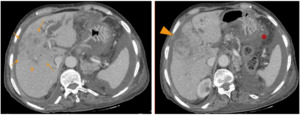
Fig. 15: Cholangiocarcinoma and peritoneal carcinomatosis.
Axial CT images in the portal phase show a peripheral mass-forming with peritoneal carcinomatosis (*). Note the capsular retraction (arrowhead).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
V-Place of percutaneous biliary drainage (PBD) in the palliative care of cholangiocarcinoma:
- This technique consists of selectively cannulating the bile duct by a percutaneous approach.
Ideally,
it leads to internal drainage with the placement of one or more stents in the biliary system.External biliary drainage is placed in case of failure to cross the stenosis or to place the stent ( Fig. 16 ,
Fig. 17 ,
Fig. 18 ,
Fig. 19 ).
- PBD is reserved for situations of failure or technical impossibility of endoscopic drainage (duodenal stenosis,
history of gastric surgery).
Bilateral obstruction or located on top of the biliary tract,
history of biliary tract surgery can also make endoscopic drainage difficult.
In case of complex peri-hilar or intra-hepatic localization,
endoscopic drainage may be ineffective,
with opacified bile ducts but undrained,
that may lead to biliary sepsis.
In this situation,
percutaneous drainage must be quickly realized.
- PBD is indicated in selected patients with severe malnutrition or biliary sepsis and in those undergoing delayed surgery due to portal vein embolization or chemoradiation therapy.
In addition,
PBD may be indicated in patients with severe pruritus or renal failure.
- The goals of the biliary drainage in the management of unresectable cholangiocarcinoma are the regression of jaundice,
the decrease of the pain and pruritus related to distention of the bile ducts and the prevention of cholangitis.
The secondary objective is a prolongation of survival.
It has been shown that the reduction of cholestasis and efficiency biliary drainage was the most powerful survival prognostic factors for inoperable perihilar cholangiocarcinoma.
Thus in patients with an unresectable cholangiocarcinoma,
the median survival is 3 months in the absence of biliary drainage of the bile ducts against 6 months in case of drainage
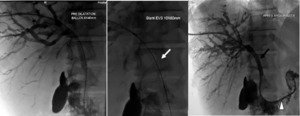
Fig. 16: Percutaneous drainage in a 42-year-old patient presenting with hilar cholangiocarcinoma (stage IV by bismuth and colorette).
-Establishment of an internal-external drainage (arrowhead).
-Placement on both sides of the stenosis of an endoprosthesis (white arrow) expanding with the help of an angioplasty balloon (black arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
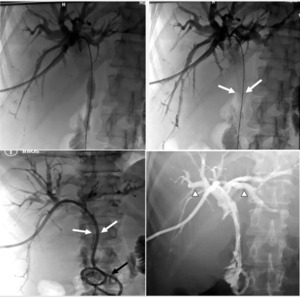
Fig. 17: Percutaneous drainage in a 69-year-old patient presenting with hilar cholangiocarcinoma (stage IV by bismuth and colorette).
Fluoroscopic images presenting following stages of placement a percutaneous transhepatic biliary drain (black arrow) and an endoprothesis (white arrow).
Note the state of biliary tracts after decompression (arrowhead).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
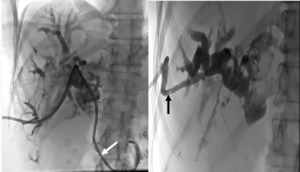
Fig. 18: Percutaneous drainage in a 60-year-old patient presenting with hilar cholangiocarcinoma (stage IV by bismuth and colorette).
The patient had previously undergone an external drainage (black arrow) because of a failure to cross the stenosis. An external-internal drainage with a right approach (white arrow) was established after 10 days.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia

Fig. 19: Bilateral percutaneous drainage in a 72-year-old patient presenting with hilar cholangiocarcinoma (stage IV by bismuth and colorette).
A : Percutaneous transhepatic cholangiography (PTC) showing a of biliary obstruction type IV of Bismuth.
B: Bilateral internal-external drainage
C: Placement of 2 stents bilaterally
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia


: 13- 26.")

 and with contrast enhancement in arterial phase (B), venous phase (C) and delayed phase (D) show a typical enhancement pattern in exophytic CC: hypointense masse before contrast administration with incomplete rim enhancement in venous phase and delayed enhancement. Note asymmetric dilation of the peripheral intrahepatic ducts surrounding the mass (arrowheads) and the capsular retraction (white arrow). References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
, in arterial phase (B), portal phase (C) and delayed phase (D) show low attenuation mass at the hepatic hilium before contrast administration with slight peripheral enhancement in the portal phase and homogenous isoattenuating mass in delayed phase. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
 and T1 post-gadolinium- (B) weighted images show a peripheral mass-forming cholangiocarcinoma (*) infiltrating the hilar area with vascular encasement and secondary important intrahepatic bile duct dilatation (red arrow). The magnetic cholangiography (C) shows a signal void (white arrow) at the confluence of the main hepatic ducts. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
 at the confluence of the main hepatic ducts (left and right), dilated bilateral intahepatic bile ducts and no dilated extrahepatic bile duct (blue marker), consistent with infiltrative hiliar CCA with proximal extension into the right and left hepatic bile ducts (Type IV of Bismuth-Corlette). References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
 and axial (C, D) CT scan images show dilated extrahepatic (blue markers) and cystic bile ducts (red markers) until the intrapancreatic portion of the common bile duct, where there is an hyperattenuated thickened wall (arrowhead). Note satellite nodule in the right hepatic lobe (white arrow). References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
 and coronal (C) T2-weighted images show a mass-forming CC infiltrating the biliary confluent and left biliary ducts (Bismuth IIIb) with vascular encasement : thrombosis of the left portal vein and extension to the common and left hepatic arteries (red arrows) with multiple metastatic hepatic nodules (arrowhead) and loco-regional lymph node extension (blue arrows). References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
 producing biliary dilatation with encasement and infiltration of the main portal vein.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
. Note the capsular retraction (arrowhead).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
.
-Establishment of an internal-external drainage (arrowhead).
-Placement on both sides of the stenosis of an endoprosthesis (white arrow) expanding with the help of an angioplasty balloon (black arrow). References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
.
Fluoroscopic images presenting following stages of placement a percutaneous transhepatic biliary drain (black arrow) and an endoprothesis (white arrow).
Note the state of biliary tracts after decompression (arrowhead). References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
.
The patient had previously undergone an external drainage (black arrow) because of a failure to cross the stenosis. An external-internal drainage with a right approach (white arrow) was established after 10 days. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
.
A : Percutaneous transhepatic cholangiography (PTC) showing a of biliary obstruction type IV of Bismuth.
B: Bilateral internal-external drainage
C: Placement of 2 stents bilaterally References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")