1) CAVERNOUS VENOUS MALFORMATION
- Previously known as "cavernous hemangioma".
- It is the most frequent benign orbital lesion in adults.
- It is a congenital vascular anomaly,
a low-flow venous malformation,
composed of dilated cavernous spaces,
covered by flattened endothelium and separated by fibrous septa,
with a well-defined capsule.
- It generally remains asymptomatic until adulthood,
so it typically presents in the fourth and fifth decades of life.
- There are cases reported presenting in childhood,
in infants with diffuse neonatal hemangiomatosis.
- About 60% of cases occur in women.
Clinical presentation:
- Progressive painless proptosis (70%) is the most common clinical sign since it is a lesion of slow growth.
- Deficits of the visual field (50%),
due to mass effect on the optic nerve.
- Other symptoms: Motility deficits,
strabismus,
and pain.
Imaging findings:
- Well-circumscribed,
ovoid and homogeneous mass most frequently located within the intraconal space.
- It tends to displace and surround adjacent structures,
being unlikely to cause a direct invasion.
CT:
- There may be bone remodeling.
Bone erosion is rare.
MRI:
- T1WI: Iso/hypointense to muscle.
- T2WI: Uniformly hyperintense (Figure 1)
- No flow voids.
- There may be internal septations.
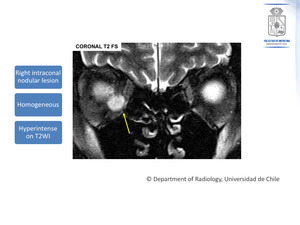
Fig. 1: Cavernous Venous Malformation. Appearance on MRI. Coronal T2 FS: A right intraconal nodular lesion is shown. It is markedly hyperintense on T2WI.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Enhancement pattern (Figure 2):
- The enhancement is poor on the early arterial phase since the mass has poor arterial supply (Patchy,
heterogeneous).
- There is progressive filling of the mass from the periphery to center on delayed venous phase images.
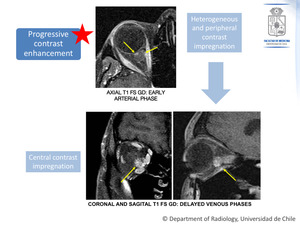
Fig. 2: Cavernous Venous Malformation. The same patient as in figure 1.
Axial, coronal and sagital T1 FS Gd images, showing the contrast enhancement pattern.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Key point:
This characteristic contrast enhancement pattern allows differentiation from vascular lesions that have rich arterial supply (such as arteriovenous malformations,
capillary hemangioma,
and solitary fibrous tumor).
2) LYMPHOPROLIFERATIVE LESIONS
- Most frequent primary orbital tumor in older adults (≥60 years of age).
- Orbital lymphoproliferative lesions comprise a wide spectrum of diseases ranging from benign to malignant lesions.
These include lymphoid hyperplasia,
atypical lymphoid hyperplasia,
and ocular adnexal lymphoma,
among others.
- They can develop as primary tumors,
or they can be a manifestation of systemic lymphoma.
- Of this spectrum,
the most common is malignant lymphoma (67%–90% of orbital lymphoproliferative tumors).
- Non-Hodgkin´s subtype MALT (mucosa-associated lymphoid tissue) is the most frequent.
Clinical presentation:
- Common signs: Palpable mass,
proptosis and mildly restricted ocular motility.
- Usually,
they are not painful.
Imaging findings:
- Usually unilateral (76%).
- Most frequently located in the extraconal space.
In 40% of cases,
the lacrimal gland is involved.
- There are mainly two forms of presentation:
- A diffuse and ill-defined lesion (50%).
- A circumscribed mass (50%).
- There is a tendency to mold to orbital structures,
such as the globe,
optic nerve,
and orbital wall.
- There may be bone remodeling.
Bone erosion is uncommon (very rare).
MRI (Figures 3,
4 and 5):
- T1WI: Isointense to muscle.
- T2WI: Relatively hypointense.
- Contrast enhancement is usually homogeneous
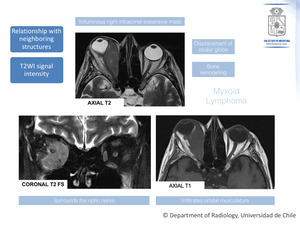
Fig. 3: An example of a lymphoproliferative lesion. In this case it corresponds to a patient with biopsy proven Myxoid Lymphoma.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
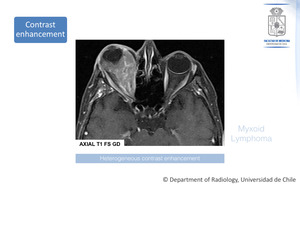
Fig. 4: Biopsy proven Myxoid Lymphoma. The same patient. Contrast enhancement appearance of the lesion is shown.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Key points:
- In differential diagnosis with pseudoturmor
- If the patient has pain,
especially an acute onset of pain,
think of pseudotumor.
- If there is tubular thickening of ocular muscles,
without infiltrative elements,
think of pseudotumor.
- The mean ADC value of orbital lymphomas is significantly lower than that of benign lymphoproliferative disorders and inflammatory diseases (Figure 5).
- It reflects higher cellularity in orbital lymphoma lesions.
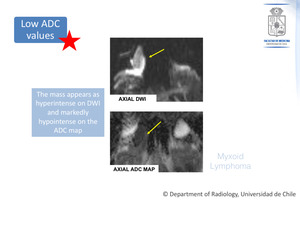
Fig. 5: Biopsy proven Myxoid Lymphoma. The same patient.
The lesion appearance on DWI and ADC map is shown.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
3) OPTIC NERVE GLIOMA:
- Optic nerve glioma is the most common primary tumor of the optic nerve.
- They can occur anywhere in the optic tract: 25-48% occur in the intraorbital segment.
Gliomas of the optic pathway can be categorized into two groups,
according to the age of presentation:
Glioma in the pediatric population:
- Relatively benign course
- Most of them are juvenile pilocytic astrocytomas (grade 1 WHO),
in children under 8 years of age (most common age of presentation).
- Composed of spindle-shaped astrocytes with hairlike (pilocytic) processes.
- There is leptomeningeal involvement,
showing reactive hyperplasia and cellular infiltration.
The dura remains intact,
which gives the fusiform appearance of the tumor.
- Most cases are sporadic,
but there is an association with neurofibromatosis type 1 (NF-1): 20% of children with NF-1 have optic nerve gliomas,
that can be bilateral.
- In 90% of cases,
the diagnosis is made before the age of 20 years.
Location
- Sporadic optic nerve gliomas are more likely to extend posteriorly to involve the optic chiasm and intracranial structures.
- Optic nerve gliomas in NF-1 patients tend to be confined to the optic nerve.
Clinical presentation:
- Patients could be asymptomatic,
being the tumor incidentally discovered (usually in patients with NF-1).
- Frequent symptoms: Variable degrees of visual field deficits,
proptosis,
afferent pupillary defect,
and strabismus.
Imaging findings (Figure 6):
- Fusiform mass centered in the optic nerve,
causing enlargement and deformity of the nerve.
In NF-1 the optic glioma could be focally tortuous,
kinked or buckled.
- It could extend posteriorly toward the chiasm,
causing enlargement of the optic canal.
MRI:
- T1WI: Usually hypointense or isointense.
- T2WI: Hyperintense.
- A hyperintense peripheral ring on T2 sequences would mean leptomeningeal infiltration.
- Contrast enhancement is variable: It could be homogenous or it could have peripheral enhancement with necrosis or cyst formation centrally.
- Calcifications are rare.
- It is important to assess the involvement of the orbital apex,
optic chiasm,
hypothalamus,
and other intracranial structures.
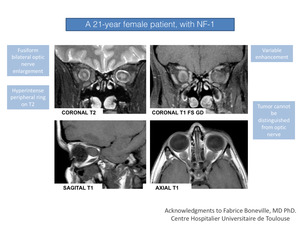
Fig. 6: A 21-year female patient, with NF-1. Contrast enhanced MRI demonstrates bilateral optic nerve gliomas.
References: Fabrice Boneville, MD PhD. Centre Hospitalier Universitaire de Toulouse.
Glioma of the adulthood:
- Extremely rare tumor
- There is no association with neurofibromatosis.
- Usually high-grade malignant neoplasms,
with aggressive behavior.
These are pathologically classified as either anaplastic astrocytoma (World Health Organization [WHO] Grade III) or glioblastoma (WHO Grade IV).
They have high mitotic activity,
necrosis,
and hemorrhage.
Clinical presentation:
Malignant neoplasms are more aggressive
- Retro-orbital pain
- Rapidly progressive vision loss (uni- or bilateral,
depending on the degree of optic chiasm involvement).
- Brain involvement could lead to focal neurological deficits.
Imaging findings:
- Expansive and infiltrative mass involving any component of the optic pathway
- Can extend to the contiguous structures.
- Variable mass effect and vasogenic edema
Key points:
The main differential diagnosis based on imaging appearance is an optic sheath meningioma,
but this is rare in children and it is seen only in the context of neurofibromatosis type 2 (not type 1) or could develop secondary to remote radiation therapy.
Another feature is that meningiomas can have calcifications.
Also keep in mind that in the case of optic nerve gliomas,
the nerve itself cannot be distinguished from the tumor.
4) OPTIC NERVE SHEATH MENINGIOMA:
- Second most frequent tumor of the optic nerve.
- 2% of all orbital masses
- Derived from the arachnoid sheath of the optic nerve.
- Primary optic nerve meningiomas are less frequent than secondary lesions that extend into the orbit from an intracranial site.
- Usually seen in adults (5th decade of life).
- Up to 80% of cases are in women.
Clinical presentation:
- In adults,
they are usually slow growing masses.
The classic symptom is a progressive and painless loss of vision.
- Proptosis is a late symptom
- In children (with NF-2) they may show signs of aggressiveness,
and could also manifest bilaterally.
Imaging findings:
Tubular growth pattern: There is segmental or diffuse circumferential thickening of the optic nerve sheath,
but the nerve itself is spared.
This is represented in two classic imaging signs that can be seen in contrast-enhanced CT or MRI (Figure 7):
- “Tram-track” sign,
on axial images: the optic nerve appears as a negative defect in relation to the surrounding enhancement of the tumor located on either side.
- “Donut” sign,
on coronal images,
reflects the same but in the coronal plane.
- Also,
neural atrophy can be seen
The mass can also manifest as a fusiform enlargement or as an eccentric mass.
CT:
- Assessment of bone remodeling
- Presence of calcifications (20-50%).
In MRI the appearance is variable in T1 and T2,
but it is the modality of choice to evaluate the extension.
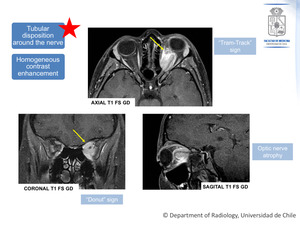
Fig. 7: Contrast enhanced MRI images, showing the classic appearance of optic nerve sheath meningioma.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Key points:
In the case of meningioma,
the tumor itself can be distinguished from the optic nerve,
contrary to what occurs in the case of gliomas,
as was previously described.
5) SCHWANNOMA:
- Also called neurilemoma.
- Benign,
encapsulated proliferation of Schwann cells,
of slow and progressive growth.
- They tend to occur in a wide range of age: 20-70 years.
Clinical presentation:
- The symptoms are nonspecific,
similar to those of the cavernous malformation.
- A perineural extension can lead to progressive symptoms,
pain and neural compression.
Imaging findings (Figures 8 and 9):
- It presents as an eccentric formation from a peripheral nerve.
- Typically extraconal and located at the superior orbit,
because the most frequent origin is in the frontal branch of the ophthalmic nerve.
- Mass of non-aggressive behavior: Displaces and compresses structures,
abuts and crosses orbital apertures.
Bone remodeling is often seen.
MRI:
- Uniform,
well-circumscribed mass.
- T1WI: Typically isointense.
- T2WI: Hyperintense and heterogeneous (solid-cystic components).
- Heterogeneous enhancement.
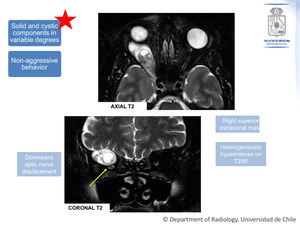
Fig. 8: Schwannoma. Lesion appearance on T2WI.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
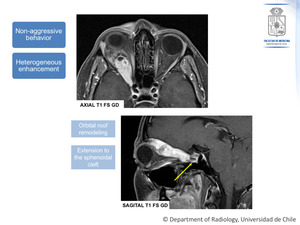
Fig. 9: Schwannoma. The same patient as figure 8.
Axial and sagital T1 FS Gd, showing the mass appearance after contrast administration.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Key points:
- The key to differential diagnosis from cavernous malformation is the enhancement pattern.
As it was previously described a progressive enhancement on delayed venous phase images favors a cavernous malformation over schwannoma.
- Also,
schwannoma tends to be more heterogeneous on T2WI because of its mixed solid and cystic composition.
