ECR 2020 / C-01389
Road the 7th nerve trods and it’s diversions
Congress:
ECR 2020
Poster Number:
C-01389
Type:
Educational Exhibit
Keywords:
Not applicable, Pathology, Diagnostic procedure, MR, CT-High Resolution, Neuroradiology brain, Neuro
Authors:
G. Ilangovan, F. Gomes, H. Balaganesan; Chennai/IN
DOI:
10.26044/ecr2020/C-01389
:571-576")
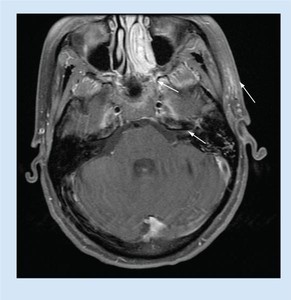
Fig. 1:
Enhancement of intracanalicular, geniculate part and left periauricular region
:571-576")
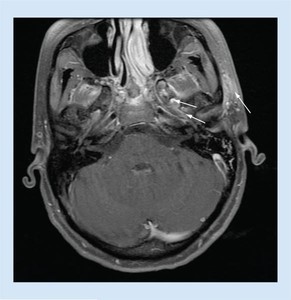
Fig. 2:
Enhancement of intracanalicular segment and periauricular region
:571-576")
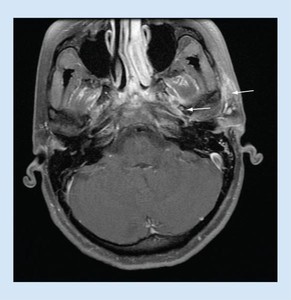
Fig. 3:
Arrows show enhancement of labrynthine segment of facial nerve and...
:571-576")
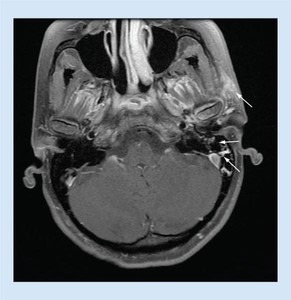
Fig. 4:
Arrows show enhancement of mastoid segment of facial nerve and left...
 lying over the atretic oval window. On the left side, the tympanic segment is more inferiorly displaced and lying over the promontory. Note the bony plate between the vestibule and the middle ear space, which enabled us to confirm the diagnosis of oval window atresia. References: Zeifer B, Sabini P, Sonne J. Congenital absence of the oval window: radiologic diagnosis and associated anomalies. AJNR Am J Neuroradiol 2000;21(2):322–327.")
Fig. 10:
Unenhanced coronal thin-section CT image of the temporal bone shows the...
 shows homogeneous enhancement of the mass (between arrows). The bone algorithm CT (right) at the same level shows focal enlargement of the descending segment with extension toward the external auditory canal (between arrows). References: The Many Faces of Facial Nerve Schwannoma. R.H. Wiggins, H.R. Harnsberger, K.L. Salzman, C. Shelton, T.R. Kertesz and C.M. Glastonbury.American Journal of Neuroradiology March 2006, 27 (3) 694-699")
Fig. 11:
Two axial images from the same case of a facial nerve schwannoma involving the...
. References: Choi JW, Park YH. Facial nerve paralysis in patients with chronic ear infections: surgical outcomes and radiologic analysis. Clinical and experimental otorhinolaryngology. 2015 Sep;8(3):218.")
Fig. 12:
Computed tomography of patient showing all semicircular canals and vestibular...