ECR 2020 / C-05136
Epistaxis: Diagnostic Approach to Common and Uncommon Causes
Congress:
ECR 2020
Poster Number:
C-05136
Type:
Educational Exhibit
Keywords:
Multicentre study, Not applicable, Neoplasia, Haematologic diseases, Foreign bodies, Imaging sequences, Diagnostic procedure, PET-CT, MR-Diffusion/Perfusion, CT-High Resolution, Vascular, Head and neck, Anatomy, Head and Neck
Authors:
E. Marín Diez1, S. Strauss2, E. YLLERA CONTRERAS3, E. M. Marco De Lucas4, C. D. Phillips2; 1Santander/ES, 2New York/US, 3BURGOS/ES, 4Santander, Ca/ES
DOI:
10.26044/ecr2020/C-05136

Fig. 3:
Etiologic factors of epistaxis.

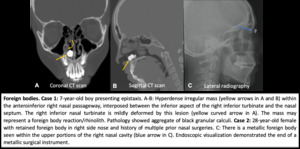
Fig. 4:
Foreign bodies.

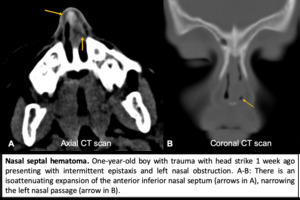
Fig. 5:
Nasal septal hematoma.

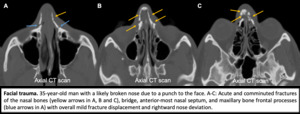
Fig. 6:
Facial trauma.

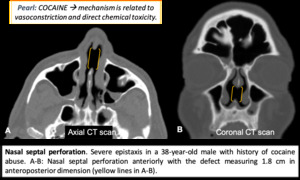
Fig. 7:
Nasal septal perforation.

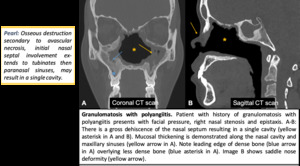
Fig. 8:
Granulomatosis with polyangiitis.

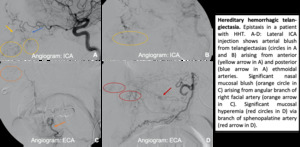
Fig. 9:
Hereditary hemorrhagic telangiectasia.

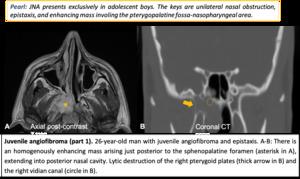
Fig. 10:
JNA
.")
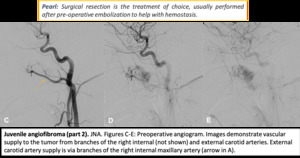
Fig. 11:
JNA (part 2).
.")
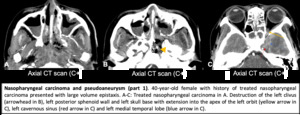
Fig. 12:
Nasopharyngeal carcinoma and pseudoaneurysm (part 1).
.")
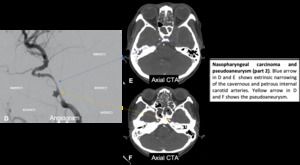
Fig. 13:
Nasopharyngeal carcinoma and pseudoaneurysm (part 2).

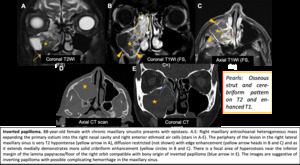
Fig. 14:
Inverted papilloma.

Fig. 15:
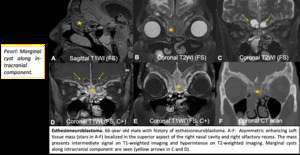
Esthesioneuroblastoma.

Fig. 16:
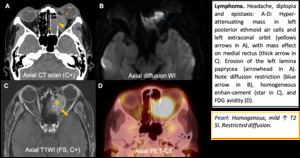
Lymphoma.

Fig. 17:
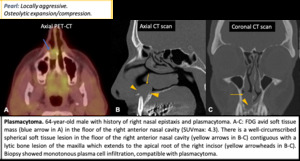
Plasmocytoma.

Fig. 18:
Summary.