ECR 2020 / C-06290
Upper gastrointestinal tract radiography: Imaging features of gastric lesions
Congress:
ECR 2020
Poster Number:
C-06290
Type:
Educational Exhibit
Keywords:
GI Tract, Abdomen, Gastrointestinal tract, Stomach (incl. Oesophagus), Fluoroscopy, Barium meal, Contrast agent-oral, Inflammation, Motility, Neoplasia, Not applicable, Performed at one institution
Authors:
S. Y. Yu, N.-C. Chiu; Taipei/TW
DOI:
10.26044/ecr2020/C-06290

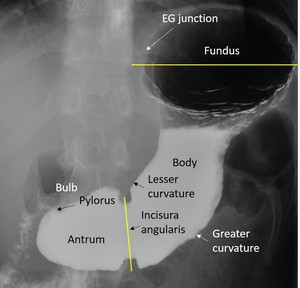
Fig. 1:
Normal anatomy of stomach on double-contrast barium study.
, also known as cardiac rosette.")
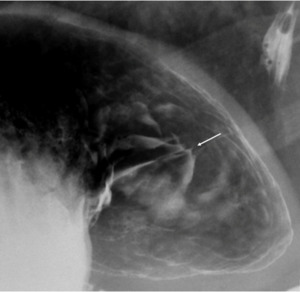
Fig. 2:
Double-contrast barium study in right anterior oblique position shows normal...

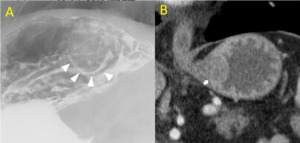
Fig. 3:
Calcification of gastric polyps
. In contrast, polyps on nondependent wall are coated by barium and appear as white lines (arrows).")
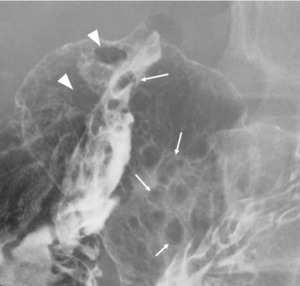
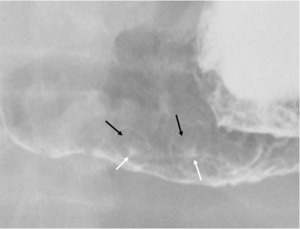
Fig. 4:
Double-contrast barium study in supine position shows multiple hyperplastic...
 collections of barium surrounded by radiolucent mounds of edema (black arrows).")
Fig. 9:
Double-contrast barium study in supine position shows erosions at gastric lower...
 with uniform fold convergence on the ulcer.")
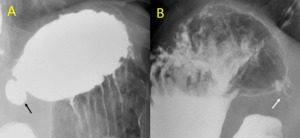
Fig. 10:
Double-contrast barium study in supine position shows benign gastric ulcer at...
 surrounded by fused and clubbed mucosal folds.")
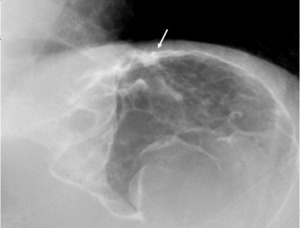
Fig. 11:
Double-contrast barium study in left posteior oblique position shows malignant...
.
B. (The same patient) Residual barium in the gastric diverticulum after barium spilled out(white arrow).")
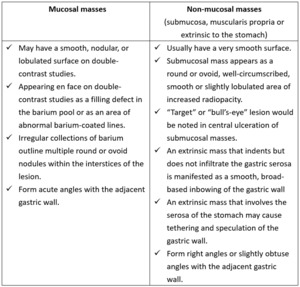
Fig. 12:
A. Double-contrast barium study in left posterior oblique position shows a...
.
B. Coronal reformat CT of the same patient shows the submucosal mass in gastric cardia(white arrow). Final pathology confirmed the diagnosis of GIST.")
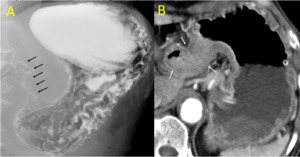
Fig. 6:
A. Double contrast barium study in right lateral position showing a...
.
B. The contrast-enhanced CT of the same patient shows irregular gastric wall thickening at antrum and pylorus with increased enhancement(white arrows). The pathology proved the final diagnosis as gastric carcinoma.")
Fig. 13:
A. Double contrast barium study in left posterior oblique position shows...
 and caustic gastric injury.")
Fig. 14:
Double contrast barium study in supine position of the patient with diffusely...

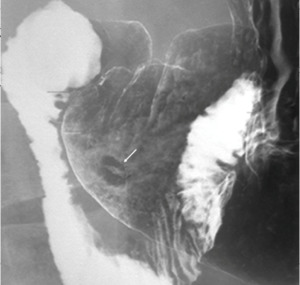
Fig. 5:
Mucosal and non-mucosal masses on double-contrast barium study
 at gastric antrum which is seen as linear collections of barium surrounded by radiolucent mounds of edema. The differential diagnosis of this image feature on double-contrast barium study could be aphthoid ulcers, mucosal or submucosal tumor with central ulceration, haematogenous gastric metastases.")
Fig. 7:
Double-contrast barium study in left posterior oblique position shows “bull's...