ECR 2020 / C-06519
Small bowel MRI: existing and new techniques
Congress:
ECR 2020
Poster Number:
C-06519
Type:
Educational Exhibit
Keywords:
Not applicable, Motility, Imaging sequences, Diagnostic procedure, MR-Enterography, MR-Diffusion/Perfusion, MR, Small bowel, Gastrointestinal tract, GI Tract
Authors:
M. Dedelaite, E. B. Mark, D. Bertoli, J. B. Frøkjær; Aalborg/DK
DOI:
10.26044/ecr2020/C-06519

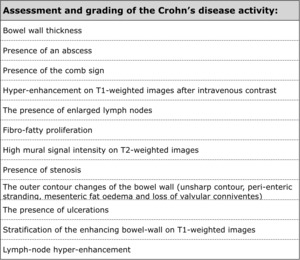
Table 1:
Assessment and grading of the Crohn’s disease activity.
 and focal thickening of ileum-wall with stenosis (black arrow) on T2-TSE coronal image.")
Fig. 1:
Mesenteric inflammation (white arrow) and focal thickening of ileum-wall with...
.")
Fig. 2:
Thickening of the ileum-wall on coronal T2-TSE image (white arrow).
 on T2-TSE coronal image.")
Fig. 3:
Significant thickening of terminal ileum with relative stenosis (white arrow)...
 on coronal T2-TSE image.")
Fig. 4:
Enlarged lymph nodes (white arrow) on coronal T2-TSE image.

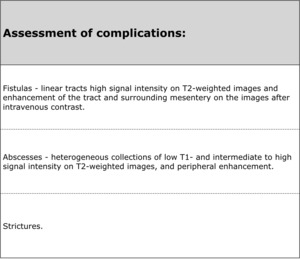
Table 2:
Assessment of complications of the Crohn's disease.
 on T2-TSE coronal image.")
Fig. 5:
Abscess (white arrow) on T2-TSE coronal image.
 of small bowel.")
Fig. 6:
Axial T2-TSE image demonstrating mural thickening and stenosis (white arrow) of...
 and ileal segment with wall-thickening and stenosis (white arrow).")
Fig. 7:
T2-TSE image showing air in the abscess cavity (yellow arrow) and ileal segment...

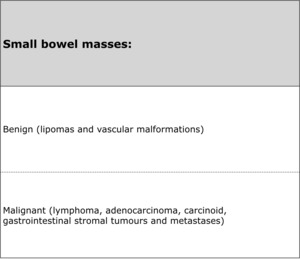
Table 3:
Small bowel masses.

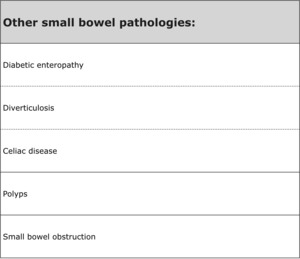
Table 4:
Other small bowel pathologies.
.")
Fig. 8:
T1-FFE image after intravenous gadolinium contrast injection shows...
 on coronal T1-FFE image after intravenous gadolinium contrast.")
Fig. 9:
Transmural enhancement (white arrow) on coronal T1-FFE image after intravenous...
 and enhancing ileal mucosa (yellow arrow).")
Fig. 10:
T1-FFE coronal image after intravenous gadolinium contrast demonstrates an...

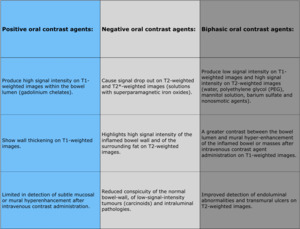
Table 5:
Oral contrast agents.
.")
Fig. 11:
T2-TSE coronal image demonstrating optimal small bowel distention (yellow...

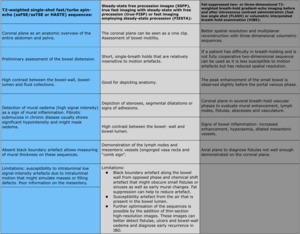
Table 6:
MR sequences.

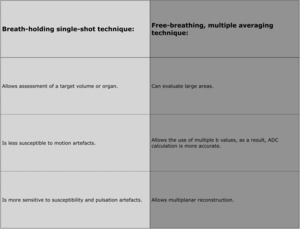
Table 7:
Breath-holding single-shot technique vs. free-breathing, multiple averaging...
 as a sign of active inflammation.")
Fig. 12:
Axial ADC-map image demonstrates diffusion restriction in the wall of distal...
 on DWI.")
Fig. 13:
Actively inflamed distal ileum demonstrating high signal intensity (yellow...